

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Dear Editor:
Angioimmunoblastic T-cell lymphoma (AITL) is an aggressive non-Hodgkin's nodal peripheral T-cell lymphoma that accounts for 18% of peripheral T-cell lymphoma, and cutaneous AITL has not been well characterized in terms of clinical and histopathologic features1. Because AITL is usually diagnosed based on lymph node biopsy, it is difficult for physicians to diagnose cutaneous AITL without lymphadenopathy.
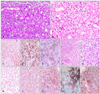
Eighty-four years old female visited our hospital with nodules on both calves. The patient claimed that she had first noticed tender nodules several months prior to the visit and that they have gradually increased in size (Fig. 1A). Examination results indicated skin-colored palpable hard nodules with tenderness, about 3.0×3.0 cm in size. The nodule histologically revealed prominent vascular proliferation surrounded by abundant epitheloid histiocytes and lymphocytes without prominent nuclear atypia in the dermis (Fig. 2A, B). There were many positive cells in CD3 and CD68 (Fig. 2C, D), foci of small aggregates of positive cells in CD31, and negative cells in S100 protein, CD1a and Epstein-Barr virus (EBV). T-cell receptor-γ gene rearrangement was found to be monoclonal. In suspicion of cutaneous T-cell lymphoma, she underwent further evaluation, such as laboratory test, whole-body computed tomography (CT), and positron emission tomography-CT in hemato-oncology. On a follow-up visit, the nodule on her left calf became a progressive ulcer with a granulation-like base (Fig. 1B). However, we could not find any evidence of infection. Inguinal lymphadenopathy was identified from imaging study, and lymph node biopsy was performed (Fig. 2F, G). Many cells in the lymph node showed positive reactions for CD3, CD4, CD5, CD21 and programmed death-1 (PD-1) (Fig. 2H~L), but negative reactions for CD8, CD20 and EBV. An additional stain for PD-1 of the skin was also positive (Fig. 2E). Based on these immunohistological findings, we were able to diagnose the skin lesion as AITL. After 6 months, she developed aggressive malignant lymphadenopathy in multiple regions of the body.
Skin involvement occurs in up to 50% of AITL patients and presents with nonspecific maculopapular eruption in most cases, but less commonly in patients with nodules1. Our patient first presented with cutaneous nodules, and histologically showed vascular proliferation with abundant histiocytic infiltration. Progressive ulceration made AITL diagnose more difficult until the lymph node biopsy result was obtained. However, PD-1 staining for the lymph node and the skin was useful in making the diagnosis2. Until now, predominant histiocytic infiltrate in cutaneous AITL such as our case has not been described. Only a few AITL cases have been reported with nodular lesion histologically showing presence of histiocytes. Although histiocytes' role in cutaneous lymphoma has been described in prominent granulomatous reaction, most cases were of mycosis fungoides3 and rare cases of AITL. CD68 has been known as negative prognostic marker for lymphoma-associated macrophage in follicular lymphoma4 and classic Hodgkin's lymphoma5. In our opinion, abundant histiocytic infiltration in cutaneous AITL may be associated with the cutaneous nodules and also with the progressive ulcer, and histiocytes might play a more aggressive role in the clinical features of AITL, which will be evaluated in the future.

 XML Download
XML Download