

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Cosmetic outcomes are becoming an increasingly important component of patient satisfaction after successful surgery. Severe scarring such as hypertrophic scar or keloids used to be the only concern, but as closure materials and techniques have advanced, minor scars are also subjected to treatment. Recent attention has focused on the scars caused by open thyroidectomy for many reasons: the site of the scar is the anterior neck, which is one of the most prominent locations of the body, the patients are mostly women, and thyroid disorders usually have good prognosis among others, to list few.
Various modalities have been used to improve the appearance of postsurgical scars or even to prevent them. Among them, laser treatment is the most preferred method because of its convenience. Pulsed-dye, ablative, and nonablative fractional lasers are the favored choices. Several studies have demonstrated their efficacy and compatibility. More recently, attention has focuses on scar prevention rather than revision or reduction.
Accordingly, this study compared the effectiveness and safety of 2 different lasers-a 595-nm pulsed-dye laser (PDL) and a 1,550-nm nonablative fractional erbium-glass laser (NAFL)-in the prevention of open thyroidectomy scars.
MATERIALS AND METHODS
Patients
Thirty adults including 3 men and 27 women aged 23~60 years with Fitzpatrick skin type III~V volunteered to participate. They had undergone open thyroidectomy performed by a single surgeon using the same surgical procedure and materials between February and July 2013. They did not have any noteworthy medical conditions besides thyroid disease or a history of keloid scars or delayed wound healing. The study was approved by the Institutional Review Board of Hallym University Sacred Heart Hospital (IRB No. 2012-I087), and all volunteers provided informed written consent prior to participation.
Treatment protocol
Starting from 2~3 weeks after open thyroidectomy, each patient received 3 sessions of laser therapy at 4-week intervals. The treatment area was gently cleansed with 70% alcohol, and 4% lidocaine (LMX4; Ferndale Laboratories Inc., Ferndale, MI, USA) was applied as a topical anesthetic cream for 30 minutes. The wound was split into halves: one half was treated with the PDL (Vbeam; Candela Laser Corporation, Wayland, MA, USA), and the other half with the NAFL (Fraxel; Solta Medical Inc., Hayward, CA, USA). Laser parameters were determined on the basis of the authors' previous experience and the literature1,2,3. The PDL had the following parameters: fluence, 8.0 J/cm2; spot size, 7 mm; pulse duration, 3 ms; spray, 30 ms; and dynamic cooling delay, 10 ms. The NAFL had 2 passes of fluence of 20 mJ and a total density of 656 microthermal treatment zones/cm2.
Assessment
Clinical photos under constant camera settings were taken before every session and 3 months after the final session. Two blinded dermatologists who were not aware of therapeutic modalities assessed the effectiveness and safety of the treatments by using the Vancouver scar scale (VSS) and visual analog scale (VAS). The VSS measures the pigmentation, vascularity, pliability, and height of scars.
Statistical analysis
The VSS score including individual and total criteria as well as the VAS score compared between laser treatments were analyzed by using Student's t-test with IBM SPSS Statistics 20.0 (IBM Co., Armonk, NY, USA). All p-values less than 0.05 were considered statistically significant.
RESULTS
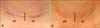
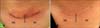
Three months after 3 sessions of PDL and NAFL on each half of the postoperative sites, the mean VSS scores improved significantly from 8.2±2.3 to 4.7±2.9 and 8.0±2.3 to 4.6±3.2, respectively (p<0.001) (Table 1, Fig. 1). Student's t-test was performed to compare the effectiveness of the 2 modalities and showed neither was inferior to the other (p=0.840; Fig. 2,3,4,5,6).
Patients were generally satisfied with both treatment sides; the VAS scores for PDL and NAFL evaluated at 6th month were 7.9±1.7 and 7.8±1.4, respectively (p=0.780; Table 1). During their treatment course, 2 patients reported erythema and itching on the PDL side after their first treatment session, but the symptoms disappeared within a week. No other adverse events such as blistering, scarring, pain, or secondary infection were observed. Three months after the final laser session, 3 patients (patients 10, 14, and 24 in Table 1) developed a hypertrophic scar on the middle portion: one each on the PDL side, NAFL side, and both sides. The degree of hypertrophy was too minor to consider any further intervention such as intralesional steroid injection, and the patients did not wish to take any additional treatment.
DISCUSSION
Postoperative surgical scars have become one of the main concerns of both patients and surgeons, but modifying surgery is insufficient to meet patients' demands. Therefore, various approaches have been developed to improve the cosmetic outcome of surgical scars. Conventional treatments included intralesional injections of steroid or 5-fluorouracil, cryotherapy, radiotherapy, silicone gel, subcision, and excisional surgery4. However, advances in therapeutic lasers have led to the development of new treatments.
Three main types of lasers are being used in the field of laser therapy: PDL, ablative fractional laser (AFL), and NAFL. PDL selectively targets hemoglobin and coagulates the microvasculature in the capillary and reticular dermis, resulting in the destruction of pathologic neovascularization5. Meanwhile, NAFL generates targeted microthermal treatment zones as well as columns of thermally denatured skin of controlled width and depth in the dermis, resulting in collagenolysis and neocollagenesis, smoothing the textural abnormalities of scarring; it can even be safely used to treat darker-pigmented patients6. Scar color, texture, morphology, and previously applied treatments are important for selecting the optimal modality and parameters7. Hypertrophic scars are commonly treated with PDL, showing remarkable results with respect to the improvement of scar erythema, pliability, bulk, and dysesthesia. Both AFL and NAFL are frequently selected for atrophic scars, producing successful outcomes with respect to skin surface texture and patient satisfaction. Ablative lasers have demonstrated better outcomes, but NAFL is popular because it is less invasive.
Ever since the abovementioned lasers were proven to be effective, research has proceeded mainly on the basis of 2 ideas: the comparative effectiveness among lasers, and laser therapy as a preventive measure. Comparing 2 modalities has been a recent trend; 2 studies have compared PDL to AFL2 and AFL to NAFL3. More studies are assumed to be in progress. Those 2 studies showed that AFL was more effective than PDL and NAFL2,3. However, the main concern with AFL still lies in its various side effects, which range from less severe ones such as acne and milia to more severe ones such as secondary infection and worsened scarring8. Various trials have aimed to clarify when to initiate therapy; some even suggest starting before the scar has developed permanently as a preventive measure. Some studies suggest laser therapy should be performed on the day of suture removal2,9. However, starting 2~3 weeks after the day of suture removal, as was performed in the present study, is gaining acceptance10.
Comparison of PDL and NAFL, as in this study have not been previously studied. Although NAFL is reported to be less effective, it is less invasive, decreasing patients' reluctance to accept treatment. Nevertheless, the present results show that both lasers were certainly effective in preventing scars, as mean VSS scores improved 3.50 and 3.37 with PDL and NAFL, respectively. The present results indicate that NAFL is as effective as PDL, a well-known authority in this field. In particular, patients reported that PDL resulted in better improvement in external appearance, while NAFL resulted in better outcomes in tactile manner; in other words, patients thought PDL helped make scars indistinguishable from the surrounding unviolated skin, but that NAFL resulted in a comparatively better in feeling of the skin with less hardening and thickening. These results may be attributable to the mechanisms of PDL, which coagulates microvasculature, thus inhibiting excessive tissue formation, and NAFL, which induces collagenolysis and neocollagenesis, reducing the fibrotic change of the scar. Further measures for objective evaluation, such as tris-stimulus analysis and narrow-band spectrophotometry for color measurement as well as ultrasonography and pneumatometry for depth and pliability measurement may be useful11.
Patients were asked if they had symptoms of pain, burning sensation, itching, redness, swelling, or oozing; no patient reported any noticeable symptoms. Although 3 patients developed hypertrophic scars 3 months after their final laser session, it is presumed to be difficult to determine which type of laser led to the development or influenced the extent of the hypertrophic scar.
In this study, 30 patients who had undergone open thyroidectomy received PDL and NAFL on each half of their postoperative sites 2~3 weeks postoperatively. There was no significant difference in outcomes between the 2 lasers according to VSS score. Moreover, patients were satisfied with both lasers, and the strength of each laser was notable.
Further studies with more subjects are required to confirm the present results. Furthermore, the development of scales that involve the measurement of induration and texture would enrich the field.





 XML Download
XML Download