

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Eccrine angiomatous hamartoma (EAH) is a benign nodular or plaque-like tumor of hamartomatous nature characterized by the proliferation of eccrine and vascular structures. It generally arises at birth or later in childhood, with a few reports of puberty- or adult-onset lesions, as solitary or multiple lesions affecting mainly the distal extremities. Hyperhidrosis and/or pain may be apparent and sometimes, hair follicles are associated with this lesion and hypertrichosis may be present. Histologically, it consists of proliferation of hyperplastic eccrine glands in association with foci of dilated capillaries at the dermal-subcutaneous level. It is a rare entity and only 17 cases have been reported in Korea. We studied 10 cases of EAH diagnosed at Ajou University Hospital and Gangnam Severance Hospital in Korea from 2007 to 2010, one of the largest single case series in the literature.
MATERIALS AND METHODS
Ten cases of EAH diagnosed at Ajou University Hospital and Gangnam Severance Hospital in Korea from 2007 to 2010 were included in this study. From the retrospective review of medical records, the patients' sex and age as well as the age of onset, location, and symptom, appearance of the lesion, and the mode of treatment were investigated. H&E stained slides from formalin fixed-paraffin embedded tissue blocks were reviewed for histopathological evaluation. Where mucin deposition was suspected, alcian blue staining at pH 2.5 was conducted. Apart from two cases where the paraffin embedded blocks unavailable, immunohistochemical staining was performed with the following antibodies: D2-40 (1:50 dilution, Cell Marque, Rocklin, CA, USA) for visualization of lymphatics, S-100 protein (1:200 dilution, Thermo Scientific, Fremont, CA, USA) for eccrine structures and neural components and factor VIII-related antige (1:100 dilution, Thermo Scientific) for delineation of vascular structures.
RESULTS
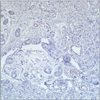
The clinical features of the patients are summarized in Table 1. The age range of patients was between 1 and 66 years (median age, 11 years) and there were an equal number of male and female patients. While two cases were congenital, others showed a late onset, ranging from 6 months to 65 years of age. Six cases developed before adolescence, and the remaining four cases had an adult onset. All of the lesions were solitary and located on the distal extremities. Nine cases appeared as a yellow-brown nodule or plaque (Fig. 1), and one case presented as a bluish nodule (Fig. 2). Three patients complained of pain and four complained of mild tenderness. In contrast to previous reports and the nature of the lesion, neither hyperhidrosis nor hypertrichosis was documented in our series. The histopathological findings were similar in all patients and were typical of EAH, exhibiting proliferation of mature eccrine and vascular structures (generally capillary) in the middle or deep dermis with normal appearing epidermis (Fig. 3, 4). There was one case showing a significant mucin deposition between eccrine coils beyond the normal extent, further confirmed by alcian blue staining. Other interesting features among the cases included the presence of fat component (patient 7) and nerve infiltration (patient 8).
Proliferated blood vessels were present in all specimens by factor VIII-related antige immunohistochemical staining, while the absence of lymphatic proliferation was confirmed by negative staining against D2-40 antigen. The eccrine apparatus in the specimens were all positive for S-100 protein at a variable intensity. Eight of the patients were referred to the plastic surgery for excision.
DISCUSSION
EAH was first described by Lotzbeck1 in 1859, from an angioma-like tumor on the face of a child. It is a rare cutaneous lesion characterized by the proliferation of multiple eccrine structures and vascular elements. The lesions generally present on an extremity at birth, or appear in early childhood, and commensurably enlarge as the patient grows. However, there is no clear explanation for the predilection for the extremities. They typically present as a solitary brownish or bluish tumor accompanied by pain and/or tenderness, but multiple lesions can occur. The lesion in patient 8 had focal neural infiltration in the dermis, which Challa and Jona2 suggested as a potential source of the discomfort and pain that accompanies EAH.
A previous article reviewed the characteristics of 15 Korean cases of EAH3. The lesions were mostly congenital (9/14, 64.2%), and although hyperhidrosis was frequent (10/15, 66.7%), they could be asymptomatic (5/15, 33.3%) or painful (6/15, 40.0%). A solitary lesion was most common (12/15, 80.0%) and the majority was a nodule (11/15, 73.3%); only three cases presented as a patch.
EAH is known to rarely arise after puberty4, although there have been a few case reports of adult-onset disease (Table 2). Interestingly, two fifths of our cases noticed the lesion in the adulthood. One possible explanation could be the absence of symptoms in those particular patients, leading to late discovery of the lesion and obscuring the actual age of onset.
EAH usually lies in the deep dermis and contains increased numbers of eccrine structures and numerous capillary channels surrounding or intermingled with the eccrine structures. The histologic criteria4 for EAH may include hyperplasia of normal or dilated eccrine glands5; close association of the eccrine structures with capillary angiomatous foci; and the variable presence of pilar, lipomatous, mucinous, and/or lymphatic structures6. In our series, pilar structures were not seen, whereas single cases showing lipomatous, mucinous and neural components were present. These hamartomatous components contribute to the external features of EAH, such as hyperhidrosis and hypertrichosis. However, neither of the symptoms was observed in our patients. Since the largest lesion in our series barely reached 15 mm in diameter, the effect of increased eccrine glands, i.e. hyperhidrosis, would not have been noticeable to the patient.
In previous immunohistochemical studies of EAH, the vascular elements stained positively for Ulex europaeus-1 and factor VIII-related antigens. The vessels were negative for glucose transporter-1 protein, supporting the hamartomatous nature of the lesion over hemangioma7. In our study, the vascular nature, rather than lymphatic, of the proliferated luminal structures in the dermis was confirmed by positive staining of the endothelial cells against factor VIII-related antiges and absence of D2-40 stained cells. The secretory portions of the eccrine glands were positive for S-100 protein, carcinoembryonic antigen, epithelial membrane antigen, and Cam5.2. The ductal components stained positively for carcinoembryonic antigen and cytokeratin 1 and weakly positive for epithelial membrane antigen8,9. These antigenic expressions were qualitatively diminished in some cases but remained comparable to normal structures10. Mitotic figures and cytologic atypia have not been observed11.
The usual clinical differential diagnoses of EAH include vascular malformations, tufted angioma, smooth muscle hamartoma, glomus tumor, blue rubber bleb nevus, and macular telangiectatic mastocytosis11,12. Interestingly, in our series, the lesions of EAH more closely resembled a callus, appearing as a yellow-brown noduloplaque located on distal extremities, where the latter condition prevails. Histopathologic examination aids distinction from these entities. However, eccrine nevus and sudoriparous angioma may display histologic resemblance. In the former, hyperplastic eccrine glands are not associated with a proliferation of capillaries. In addition, most eccrine nevi demonstrate hyperhidrosis, in contrast to approximately one third of documented cases of EAH6. Sudoriparous angioma is a related entity in which the angiomatous component predominates and the eccrine elements are dilated but not hyperplastic5,13. In EAH, the vessels are capillary in nature6, whereas in sudoriparous angioma, the vessels are predominantly large-caliber5,14,15.
In summary, our cases were typical of EAH in histopathology, demonstrating proliferation of eccrine and vascular structures. However, the frequent occurrence in the adulthood and absence of symptoms may distinguish our series from previous reports. Also, the close resemblance to callosities in our series warrants skin biopsy whenever the diagnosis is doubtful.





 XML Download
XML Download