

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Recent developments in biomechanics and technology have improved our understanding of the shoulder joints. While the shoulder joint is the one of the most mobile joints in the human body, its stability mostly relies on soft tissue structures such as the glenoid labrum and capsular ligament. Traumatic anterior instability is the most common instability related to sports injury. Younger individuals have a higher rate of recurrence after nonoperative treatment after the first-time episode of anterior instability. Arthroscopic repair of the Bankart lesion provides reliable outcomes in most of the anterior instability, while selected patients with significant bone loss may require bony augmentation procedures. Posterior instability has been underestimated. Sports injury is commonly associated with symptomatic posterior instability, and posterior labral lesions are commonly found. Arthroscopic reconstruction of the posteroinferior height and ligament balance is required. Superior labral lesions are a commonly diagnosed disease in the shoulder. Care must be taken to avoid unnecessary surgical procedures especially in nonathletic populations without significant traumatic episodes. Partial articular surface tears are common among sports related rotator cuff injuries. Symptomatic articular surface tears require arthroscopic treatment such as debridement or trans-tendon repair.
Figures and Tables
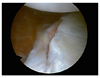
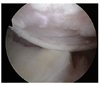

Figure 4
The jerk test. (A) Stabilize the scapula with one hand, while the other hand holds the elbow with the arm in 90° abduction and internal rotation. Firm axial compression force is applied on the glenohumeral joint. (B) The arm is horizontally adducted while maintaining the firm axial load.

Figure 5
The Kim test was performed in sitting position with the arm in 90° abduction. (A) With examiner holding elbow and lateral aspect of the proximal arm, firm axial loading force is applied. (B) Simultaneous 45° upward diagonal elevation was applied on the distal arm, while downward and backward force is applied on the proximal arm.

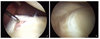
Figure 6
Three types of the posteroinferior labral lesion in the magnetic resonance imaging-arthrogram. (A) Type I: separation without displacement. (B) Type II: incomplete avulsion-the Kim lesion. (C) Type III: loss of contour.




References
1. Robinson CM, Howes J, Murdoch H, Will E, Graham C. Functional outcome and risk of recurrent instability after primary traumatic anterior shoulder dislocation in young patients. J Bone Joint Surg Am. 2006. 88:2326–2336.

2. Bottoni CR, Wilckens JH, DeBerardino TM, D'Alleyrand JC, Rooney RC, Harpstrite JK, Arciero RA. A prospective, randomized evaluation of arthroscopic stabilization versus nonoperative treatment in patients with acute, traumatic, first-time shoulder dislocations. Am J Sports Med. 2002. 30:576–580.
3. Kirkley A, Griffin S, Richards C, Miniaci A, Mohtadi N. Prospective randomized clinical trial comparing the effectiveness of immediate arthroscopic stabilization versus immobilization and rehabilitation in first traumatic anterior dislocations of the shoulder. Arthroscopy. 1999. 15:507–514.
4. Mizuno N, Yoneda M, Hayashida K, Nakagawa S, Mae T, Izawa K. Recurrent anterior shoulder dislocation caused by a midsubstance complete capsular tear. J Bone Joint Surg Am. 2005. 87:2717–2723.
5. Barnes CJ, Getelman MH, Snyder SJ. Results of arthroscopic revision anterior shoulder reconstruction. Am J Sports Med. 2009. 37:715–719.
6. Bottoni CR, Smith EL, Berkowitz MJ, Towle RB, Moore JH. Arthroscopic versus open shoulder stabilization for recurrent anterior instability: a prospective randomized clinical trial. Am J Sports Med. 2006. 34:1730–1737.
7. Kim SH, Ha KI, Kim SH. Bankart repair in traumatic anterior shoulder instability: open versus arthroscopic technique. Arthroscopy. 2002. 18:755–763.
8. Kim SH, Ha KI, Cho YB, Ryu BD, Oh I. Arthroscopic anterior stabilization of the shoulder: two to six-year follow-up. J Bone Joint Surg Am. 2003. 85-A:1511–1518.
9. Mazzocca AD, Brown FM Jr, Carreira DS, Hayden J, Romeo AA. Arthroscopic anterior shoulder stabilization of collision and contact athletes. Am J Sports Med. 2005. 33:52–60.
10. Kim SH, Park JC, Park JS, Oh I. Painful jerk test: a predictor of success in nonoperative treatment of posteroinferior instability of the shoulder. Am J Sports Med. 2004. 32:1849–1855.
11. Kim SH, Park JS, Jeong WK, Shin SK. The Kim test: a novel test for posteroinferior labral lesion of the shoulder--a comparison to the jerk test. Am J Sports Med. 2005. 33:1188–1192.
12. Kim SH, Ha KI, Park JH, Kim YM, Lee YS, Lee JY, Yoo JC. Arthroscopic posterior labral repair and capsular shift for traumatic unidirectional recurrent posterior subluxation of the shoulder. J Bone Joint Surg Am. 2003. 85-A:1479–1487.
13. Kim SH, Ha KI, Yoo JC, Noh KC. Kim's lesion: an incomplete and concealed avulsion of the posteroinferior labrum in posterior or multidirectional posteroinferior instability of the shoulder. Arthroscopy. 2004. 20:712–720.
14. Kim SH, Kim HK, Sun JI, Park JS, Oh I. Arthroscopic capsulolabroplasty for posteroinferior multidirectional instability of the shoulder. Am J Sports Med. 2004. 32:594–607.
15. Bigliani LU, Kurzweil PR, Schwartzbach CC, Wolfe IN, Flatow EL. Inferior capsular shift procedure for anterior-inferior shoulder instability in athletes. Am J Sports Med. 1994. 22:578–584.
16. Tibone JE, Bradley JP. The treatment of posterior subluxation in athletes. Clin Orthop Relat Res. 1993. (291):124–137.
17. Rhee YG, Lee DH, Lim CT. Posterior capsulolabral reconstruction in posterior shoulder instability: deltoid saving. J Shoulder Elbow Surg. 2005. 14:355–360.
18. Misamore GW, Facibene WA. Posterior capsulorrhaphy for the treatment of traumatic recurrent posterior subluxations of the shoulder in athletes. J Shoulder Elbow Surg. 2000. 9:403–408.
19. Burkhart SS, Morgan CD. The peel-back mechanism: its role in producing and extending posterior type II SLAP lesions and its effect on SLAP repair rehabilitation. Arthroscopy. 1998. 14:637–640.
20. Snyder SJ, Karzel RP, Del Pizzo W, Ferkel RD, Friedman MJ. SLAP lesions of the shoulder. Arthroscopy. 1990. 6:274–279.
21. Kim SH, Ha KI, Ahn JH, Kim SH, Choi HJ. Biceps load test II: a clinical test for SLAP lesions of the shoulder. Arthroscopy. 2001. 17:160–164.
22. Snyder SJ, Banas MP, Karzel RP. An analysis of 140 injuries to the superior glenoid labrum. J Shoulder Elbow Surg. 1995. 4:243–248.
23. Kim SH, Ha KI, Kim SH, Choi HJ. Results of arthroscopic treatment of superior labral lesions. J Bone Joint Surg Am. 2002. 84-A:981–985.
24. Burkhart SS, Morgan C. SLAP lesions in the overhead athlete. Orthop Clin North Am. 2001. 32:431–441. viii
25. Lo IK, Burkhart SS. Transtendon arthroscopic repair of partial-thickness, articular surface tears of the rotator cuff. Arthroscopy. 2004. 20:214–220.
26. Gonzalez-Lomas G, Kippe MA, Brown GD, Gardner TR, Ding A, Levine WN, Ahmad CS. In situ transtendon repair outperforms tear completion and repair for partial articular-sided supraspinatus tendon tears. J Shoulder Elbow Surg. 2008. 17:722–728.
27. Ide J, Maeda S, Takagi K. Arthroscopic transtendon repair of partial-thickness articular-side tears of the rotator cuff: anatomical and clinical study. Am J Sports Med. 2005. 33:1672–1679.
 XML Download
XML Download