

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Given the continuous advances in the hardware and software of magnetic resonance imaging (MRI), cardiac MRI has come to be a routine imaging modality in clinical settings for evaluating both cardiac function and anatomy in various cardiovascular diseases. Recently, 3 tesla (T) MRI has become available and has demonstrated advantages over 1.5T in a broad range of clinical applications although some technical challenges still remain. This review will focus on the potential advantages and limitations of 3T cardiac MRI and its current clinical applications.
Figures and Tables
Figure 1
Short axis cine images acquired at 3 tesla magnetic resonance imaging. (A) Balanced steady-state free-precession (bSSFP) cine image shows dark-band artifact (arrows) caused by B0 inhomogeneity, especially in the lateral and inferior wall of the left ventricle at the heart-lung interface. (B) Spoiled gradient echo sequence image obtained from the same patient in (A) demonstrates no such dark-band artifact though contrast between myocardium and ventricular cavity is somewhat low compared to bSSFP cine image. (C) bSSFP cine image obtained from another patient with local shimming and 32 channel cardiac coil shows excellent image quality without dark-band artifact.

Figure 2
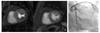
First-pass perfusion image acquired at 3 tesla magnetic resonance imaging (MRI). A 74 year-old man with typical angina underwent stress perfusion MRI. First-pass perfusion MRI during adenosine stress (A) shows subendocardial perfusion defect at the lateral and inferior wall of the left ventricle while perfusion image at resting state (B) demonstrates no perfusion defect. Coronary angiography revealed critical stensosis at the middle segment of the left circumflex arery.


References
1. Wen H, Denison TJ, Singerman RW, Balaban RS. The intrinsic signal-to-noise ratio in human cardiac imaging at 1.5, 3, and 4T. J Magn Reson. 1997. 125:65–71.

2. Wiesinger F, Boesiger P, Pruessmann KP. Electrodynamics and ultimate SNR in parallel MR imaging. Magn Reson Med. 2004. 52:376–390.
3. Bammer R, Schoenberg SO. Current concepts and advances in clinical parallel magnetic resonance imaging. Top Magn Reson Imaging. 2004. 15:129–158.
4. Hays AG, Schär M, Kelle S. Clinical applications for cardiovascular magnetic resonance imaging at 3 tesla. Curr Cardiol Rev. 2009. 5:237–242.
5. Lohan DG, Saleh R, Tomasian A, Krishnam M, Finn JP. Current status of 3-T cardiovascular magnetic resonance imaging. Top Magn Reson Imaging. 2008. 19:3–13.
6. Tyler DJ, Hudsmith LE, Petersen SE, Francis JM, Weale P, Neubauer S, Clarke K, Robson MD. Cardiac cine MR-imaging at 3T: FLASH vs SSFP. J Cardiovasc Magn Reson. 2006. 8:709–715.
7. Deshpande VS, Shea SM, Li D. Artifact reduction in true-FISP imaging of the coronary arteries by adjusting imaging frequency. Magn Reson Med. 2003. 49:803–809.
8. Wieben O, Francois C, Reeder SB. Cardiac MRI of ischemic heart disease at 3 T: potential and challenges. Eur J Radiol. 2008. 65:15–28.
9. Nael K, Fenchel M, Saleh R, Finn JP. Cardiac MR imaging: new advances and role of 3T. Magn Reson Imaging Clin N Am. 2007. 15:291–300.
10. Fenchel M, Kramer U, Nael K, Miller S. Cardiac magnetic resonance imaging at 3.0 T. Top Magn Reson Imaging. 2007. 18:95–104.
11. Cheng AS, Pegg TJ, Karamitsos TD, Searle N, Jerosch-Herold M, Choudhury RP, Banning AP, Neubauer S, Robson MD, Selvanayagam JB. Cardiovascular magnetic resonance perfusion imaging at 3-tesla for the detection of coronary artery disease: a comparison with 1.5-tesla. J Am Coll Cardiol. 2007. 49:2440–2449.
12. Zerhouni EA, Parish DM, Rogers WJ, Yang A, Shapiro EP. Human heart: tagging with MR imaging: a method for noninvasive assessment of myocardial motion. Radiology. 1988. 169:59–63.
13. Fischer SE, McKinnon GC, Maier SE, Boesiger P. Improved myocardial tagging contrast. Magn Reson Med. 1993. 30:191–200.
14. Kramer U, Deshpande V, Fenchel M, Klumpp B, Laub G, Finn JP, Claussen CD, Miller S. Cardiac MR tagging: optimization of sequence parameters and comparison at 1.5 T and 3.0 T in a volunteer study. Rofo. 2006. 178:515–524.
15. Yang Q, Li K, Liu X, Bi X, Liu Z, An J, Zhang A, Jerecic R, Li D. Contrast-enhanced whole-heart coronary magnetic resonance angiography at 3.0-T: a comparative study with X-ray angiography in a single center. J Am Coll Cardiol. 2009. 54:69–76.
16. Sommer T, Hackenbroch M, Hofer U, Schmiedel A, Willinek WA, Flacke S, Gieseke J, Träber F, Fimmers R, Litt H, Schild H. Coronary MR angiography at 3.0 T versus that at 1.5 T: initial results in patients suspected of having coronary artery disease. Radiology. 2005. 234:718–725.
17. Maintz D, Ozgun M, Hoffmeier A, Quante M, Fischbach R, Manning WJ, Heindel W, Botnar RM. Whole-heart coronary magnetic resonance angiography: value for the detection of coronary artery stenoses in comparison to multislice computed tomography angiography. Acta Radiol. 2007. 48:967–973.
18. Pouleur AC, le Polain de Waroux JB, Kefer J, Pasquet A, Vanoverschelde JL, Gerber BL. Direct comparison of whole-heart navigator-gated magnetic resonance coronary angiography and 40-and 64-slice multidetector row computed tomography to detect the coronary artery stenosis in patients scheduled for conventional coronary angiography. Circ Cardiovasc Imaging. 2008. 1:114–121.
 XML Download
XML Download