

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Figures and Tables
Fig. 1
Stability of fixation and type of healing of the fracture.
(A) Absolute stability creates a low strain environment conductive to direct bone healing.
(B) Relative stability creates an environment conductive to indirect bone healing.
(C) High strain conditions create a situation where the gap elongation exceeds tissue compliance, which can lead to cell rupture and cessation of healing.

Fig. 2
The tolerance of instability of a simple fracture versus a multifragmentary fracture.
The initial gap width of each fracture line (5 mm) and the overall displacement are the same (5 mm) in (A) and (B). In a simple transverse fracture (A) the full amount of the displacement (5 mm) is active within a fracture gap. This is equal to 100% strain, which is the limit of tolerated strain for granulation tissue. But in a multifragmentary fracture with five gaps (B) the gaps share the overall displacement. Thus, each displaces from 5 mm to 6 mm, and the resulting strain is only 20%.

Fig. 3
Influence of screw placement relative to the fracture site, the working length.
(A) The plate stress within the short working length is higher.
(B) The plate stress within the longer working length is lower.

Fig. 4
Effective usage of plate length.
The farthest screws determine the effective usage of plate length and contribute to fracture gap stability. A long plate (A) produces markedly less pull-out force than a short plate (B).

Fig. 5
Effect of plate length on screw loading.
For a given amount of bending moment a longer plate (A) produces markedly less pull-out force than a short plate (B) due to an improvement of the working leverage for the screws.

Fig. 6
Importance of cortical thickness on the working length of monocortical screws and improvement of the working length in osteoporotic bone.
(A) In normal bone the working length of a monocortical screw is sufficient.
(B) In osteoporotic bone the working length of a monocortical screw is insufficient due to the thin cortex, and under torque the bone thread will wear out soon and instability will occur.
(C) In osteoporotic bone the standard use of bicortical screws enhances the working length leading to much higher torque resistance.

Fig. 7
Fracture of the femur in a 17-year-old adolescent male.
(A) The initial x-rays showed a fracture of the femoral shaft with small bony fragments.
(B) MIPO was performed with a broad LC-DCP to avoid potential complication of avascular necorsis of the femoral head after IM nailing in adolescents.
(C) The fracture was healed with solid callus formation.
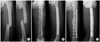
Fig. 8
Pull-out strength of regular screws and locking screws under bending load.
(A) The regular screws are pulled out sequently as a result of a bending load.
(B) The pull-out strength of locking screws against a bending load is higher due to the larger resistance area.

Fig. 9
Combi-hole of LCP (B).
One half of the hole is the dynamic compression unit for a standard screw (A) (black arrow). The other half is conical and threaded to accept the matching thread of the locking head screw (C) in order to provide angular stability (empty arrow).

Fig. 10
Diagrams showing improved anchorage of divergent locked screws.
Locked screws with divergent inclination each other (A) improve the anchorage because more bone must be displaced than parallel or non-locked screws (B) when pullout load is applied.

Fig. 11
Complex fracture of the proximal tibia in a 66-year-old male.
(A) The initial x-rays showed a segmental comminuted fracture of the proximal tibia involving the articular surface.
(B) A LCP-PLT was inserted into the submuscular, extraperiosteal tunnel through a small proximal incision. After reducing the fracture indirectly by manual traction proximal and distal screws were inserted.
(C) Then standard cortex screws were inserted percutaneously to pull the middle fragment to the plate.
(D) Postoperative x-rays showed good alignment of the fracture and stable fixation.

Fig. 12
Complex fracture of the humeral shaft in a 45-year-old female.
(A) The initial x-rays showed a segmental comminuted fracture of the humeral shaft involving the proximal humerus.
(B) As preoperative planning the fracture fragments were drawn separately on the drawing of the normal side The planned metaphyseal plate twisted as a helix was superimposed and drawn in an optimal position.
(C) The helical plate was inserted into the submuscular, extraperiosteal tunnel. After reducing the fracture indirectly screws were inserted according to the preoperative planning.
(D) Postoperative x-rays showed good alignment of the fracture and stable fixation.
(E) Follow-up x-rays 6 months after surgery showed good fracture healing with callus formation.

Fig. 13
Simple fracture of the humeral shaft in a 25-year-old male.
(A) The initial x-rays showed a simple transverse fracture of the mid-shaft of the humerus.
(B) MIPO was achieved by indirect reduction and biological fixation with a LCP through small incisions.
(C) Postoperative x-rays showed good alignment of the fracture and stable fixation.
(D) Follow-up x-rays 10 months after surgery showed good fracture healing with callus formation.

Fig. 14
Plate span ratio and plate screw density in bridge plating technique.
The plate span ratio is the quotient of plate length and overall fracture length. The plate screw density is the quotient formed by the number of screws inserted and the number of plate holes.

Fig. 15
Fracture of the distal tibia in a 33-year-old male.
(A) Initial x-rays showed a simple fracture of the distal tibia.
(B) A premeasured and precontoured metaphyseal LCP was inserted, using the threaded drill guide as a handle, into a subcutaneous tunnel. The fracture was reduced indirectly by use of a supporting pad, manual traction and use of pointed reduction forceps percutaneously.
(C) The first screw was inserted at the distal end of the plate closed to the joint line and the second screw was inserted percutaneously at the proximal end of the plate. After confirming the fracture reduction, a lag screw was inserted through the plate to reduce the fracture gap. The remaining screws were inserted according to the preoperative planning.
(D) Postoperative x-rays showed satisfactory reduction and stable fixation with a metaphyseal LCP.
(E) Follow-up x-rays 6 months after surgery showed good fracture healing with external callus.

Fig. 16
Tightening of the first LHS without stabilization of the other end of the plate will cause the "helicopter effect".

Fig. 17
Lesser trochanter shape sign.
(A) Intact opposite side: Before positioning the patient, the shape of the lesser trochanter of the intact side with the patella facing anteriorly is stored in the image intensifier.
(B) In correct rotational alignment, the shape of the lesser trochanter is symmetrical with the stored image of the intact side.
(C) In external rotation deformity, the lesser trochanter is smaller and partially hidden behind the proximal femoral shaft.
(D) In internal rotation deformity, the lesser trochanter is enlarged.

Fig. 18
Radiological signs of malrotation depending on the cortical thickness and the bone diameter.
(A) Cortical step sign: In the presence of a considerable rotational deformity, the cortices of the proximal and distal main fragments appear to have different thickness.
(B) Diameter difference sign: This sign is positive at levels where the bone cross section is oval rather than round. With malrotation, the diameters of main fragments appear to be of different sizes.

Fig. 19
Radiological assessment of rotation of the tibia with comparison of the shape of the proximal and distal tibiofibular joints and the position of the patella with the contralateral side.
(A) Intact opposite side: The shape of the tibiofibular joints and the position of the patella on the intact side.
(B) Correct rotational alignment: The shape of the tibiofibular joint and the position of the patella are the same as those of the intact opposite side.
(C) Internal malrotation: The tibia and fibula in the proximal joint are more overlapped and the patella is displaced laterally.
(D) External rotation: The tibia and fibula in the proximal joint are less overlapped and the patella is displaced medially.

Fig. 20
Cable technique for checking alignment in the frontal plane.
A cable is spanned between the center of the femoral head and the center of the ankle joint (A). The position of the cable relative to the center of the knee joint under image intensifier indicates the axial deviation in the frontal plane (B; correct alignment, C; axial deviation).

References
1. Apivatthakakul T, Arpornchayanon O, Bavornratanavech S. Minimally invasive plate osteosynthesis (MIPO) of the humeral shaft fracture. Is it possible? A cadaveric study and preliminary report. Injury. 2005; 36:530–538.

2. Baumgaertel F, Buhl M, Rahn BA. Fracture healing in biological plate osteosynthesis. Injury. 1998; 29:Suppl 3. C3–C6.
3. Byun YS, Shin DJ, Chang SA, Kwon DY. Inlay fibular autograft and helical LCP fixation for a segmental comminuted fracture of the osteoporotic proximal humerus: a case report. J Korean Fract Soc. 2006; 19:100–103.
4. Chang SA, Ahn HS, Byun YS, Kim JH, Bang HH, Kwon DY. Minimally invasive plate osteosynthesis in unstable fractures of the distal tibia. J Korean Fract Soc. 2005; 18:155–159.
5. Cheal EJ, Mansmann KA, DiGioia AM 3rd, Hayes WC, Perren SM. Role of interfragmentary strain in fracture healing: ovine model of a healing osteotomy. J Orthop Res. 1991; 9:131–142.
6. Collinge C, Sanders R, DiPasquale T. Treatment of complex tibial periarticular fractures using percutaneous techniques. Clin Orthop Relat Res. 2000; 375:69–77.
7. Deangelis JP, Deangelis NA, Anderson R. Anatomy of the superficial peroneal nerve in relation to fixation of tibia fractures with the less invasive stabilization system. J Orthop Trauma. 2004; 18:536–539.
8. Egol KA, Kubiak EN, Fulkerson E, Kummer FJ, Koval KJ. Biomechanics of locked plates and screws. J Orthop Trauma. 2004; 18:488–493.
9. Farouk O, Krettek C, Miclau T, Schandelmaier P, Guy P, Tscherne H. Minimally invasive plate osteosynthesis and vascularity: preliminary results of a cadaver injection study. Injury. 1997; 28:Suppl 1. A7–A12.
10. Farouk O, Krettek C, Miclau T, Schandelmaier P, Guy P, Tscherne H. Minimally invasive plate osteosynthesis: does percutaneous plating disrupt femoral blood supply less than the traditional technique? J Orthop Trauma. 1999; 13:401–406.
11. Fernandez Dell'Oca AA. The principle of helical implants. Unusual ideas worth considering. Injury. 2002; 33:Suppl 1. SA1–SA27.
12. Frigg R. Development of the locking compression plate. Injury. 2003; 34:Suppl 2. B6–B10.
13. Frigg R. Locking compression plate (LCP). An osteosynthesis plate based on the dynamic compression plate and the point contact fixator (PC-Fix). Injury. 2001; 32:Suppl 2. 63–66.
14. Frigg R, Appenzeller A, Christensen R, Frenk A, Gilbert S, Schavan R. The development of the distal femur less invasive stabilization system. Injury. 2001; 32:Suppl 3. SC24–SC31.
15. Gautier E, Rahn BA, Perren SM. Vascular remodelling. Injury. 1995; 26:Suppl 2. 11–19.
16. Gautier E, Sommer C. Guidelines for the clinical application of the LCP. Injury. 2003; 34:Suppl 2. B63–B76.
17. Goodship AE, Kenwright J. The influence of induced micromovement upon the healing of experimental tibial fractures. J Bone Joint Surg Br. 1985; 67:650–655.
18. Kim JJ, Kim EG, Choi JW, Park SS. Prediction of rotationally neutral state of the femur by comparing with the shape of contra-lateral lesser trochanter. J Korean Orthop Assoc. 1999; 34:899–903.
19. Kinast C, Bolhofner BR, Mast JW, Ganz R. Subtrochanteric fractures of the femur Results of treatment with the 95 degrees condylar blade-plate. Clin Orthop Relat Res. 1989; 238:122–130.
20. Krettek C, Miclau T, Grun O, Schandelmaier P, Tscherne H. Intraoperative control of axes, rotation and length in femoral and tibial fractures Technical note. Injury. 1998; 29:C29–C39.
21. Krettek C, Miclau T, Stephan C, Tscherne H. Transarticular approach and retrograde plate osteosynthesis for complex distal intraarticular femur fractures. Techniques Orthop. 1999; 14:219–229.
22. Krettek C, Rudolf J, Schandelmaier P, Guy P, Konemann B, Tscherne H. Unreamed intramedullary nailing of femoral shaft fractures: operative technique and early clinical experience with the standard locking option. Injury. 1996; 27:233–254.
23. Krettek C, Schandelmaier P, Miclau T, Tscherne H. Minimally invasive percutaneous plate osteosynthesis (MIPPO) using the DCS in proximal and distal femoral factures. Injury. 1997; 28:Suppl 1. A20–A30.
24. Kubiak EN, Fulkerson E, Strauss E, Egol KA. The evolution of locked plates. J Bone Joint Surg Am. 2006; 88:Suppl 4. 189–200.
25. Laurence M, Freeman MA, Swanson SA. Engineering considerations in the internal fixation of fractures of the tibial shaft. J Bone Joint Surg Br. 1969; 51:754–768.
26. Mast J, Jacob R, Ganz R. Planning and reduction technique in fracture surgery. 1st ed. Berlin; Heidelberg; New York: Springer-Verlag;1989. p. 11–47. p. 48–129. p. 130–200.
27. Miclau T, Martin RE. The evolution of modern plate osteosynthesis. Injury. 1997; 28:Suppl 1. A3–A6.
28. Oh CW. Treatment of complex distal tibial fractures. J Korean Fract Soc. 2005; 18:485–490.
29. Perren SM. Backgrounds of the technology of internal fixators. Injury. 2003; 34:Suppl 2. B1–B3.
30. Perren SM. Evolution and rationale of locked internal fixator technology. Introductory remarks. Injury. 2001; 32:Suppl 2. B3–B9.
31. Perren SM. Evolution of the internal fixation of long bone fractures. The scientific basis of biological internal fixation: choosing a new balance between stability and biology. J Bone Joint Surg Br. 2002; 84:1093–1110.
32. Perren SM. The concept of biological plating using the limited contact-dynamic compression plate (LC-DCP). Scientific background, design and application. Injury. 1991; 22:Suppl 1. 1–41.
33. Perren SM, Cordey J, Rahn BA, Gautier E, Schneider E. Early temporary porosis of bone induced by internal fixation implants. A reaction to necrosis, not to stress protection. Clin Orthop Relat Res. 1988; 232:139–151.
34. Rahn BA, Gallinaro P, Baltensperger A, Perren SM. Primary bone healing. An experimental study in the rabbit. J Bone Joint Surg Am. 1971; 53:783–786.
35. Rozbruch RS, Muller U, Gautier E, Ganz R. The evolution of femoral shaft plating technique. Clin Orthop Relat Res. 1998; 354:195–208.
36. Ruedi TP, Murphy WM. AO principles of fracture management. 1st ed. Stuttgart; New York: Thieme;2000. p. 7–31. p. 139–155. p. 169–184. p. 195–218. p. 221–230. p. 249–253. p. 290–305.
37. Schatzker J. Changes in the AO/ASIF principles and methods. Injury. 1995; 26:51–56.
38. Schutz M, Muller M, Krettek C, et al. Minimally invasive fracture stabilization of distal femoral fractures with the LISS: a prospective multicenter study. Results of a clinical study with special emphasis on difficult cases. Injury. 2001; 32:Suppl 3. SC48–SC54.
39. Stannard JP, Wilson TC, Volgas DA, Alonso JE. Fracture stabilization of proximal tibial fractures with the proximal tibial LISS: early experience in Birmingham, Alabama (USA). Injury. 2003; 34:Suppl 1. A36–A42.
40. Stoffel K, Dieter U, Stachowiak G, Gachter A, Kuster MS. Biomechanical testing of the LCP - how can stability in locked internal fixators be controlled. Injury. 2003; 34:Suppl 2. B11–B19.
41. Tepic S, Perren SM. The biomechanics of the PC-Fix internal fixator. Injury. 1995; 26:5–10.
42. Tong GO, Bavonratanavech S. AO manual of fracture management. Minimally invasive plate osteosynthesis (MIPO). 1st ed. Stuttgart: Thieme;2007. p. 3–45. p. 66–118. p. 305–325.
43. Wagner M. General principles for the clinical use of the LCP. Injury. 2003; 34:Suppl 2. B31–B42.
44. Yang KH, Han DY, Park SJ, Yoo HW. Spiral plate fixation for treatment of proximal humerus fracture. J Korean Orthop Assoc. 2000; 35:71–76.
 XML Download
XML Download