

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
Since its introduction in the mid-1990s, sentinel lymph node biopsy has been rapidly and widely adopted for the axillary staging of clinically node-negative breast cancer patients. However, there is some controversy in the clinical application because of its various identification rates and its false negative rates. The objective of this study was to assess the usefulness of endoscopic sentinel lymph node biopsy (ESNB) and to compare the value of two methods for identification of ESNB using blue dye only or a combination of blue dye and radioisotope.
Methods
This study was carried out in 137 breast cancer patients (bilateral breast cancer, 3 cases) who underwent ESBN, at the Department of Surgery in Soonchunhyang University from May of 2007 to August of 2008. The technique involved the injection of 5 mL of 0.5% indigocarmine or Tc-99m tin colloid into subareolar plexus. The Visiport docked with a telescope was inserted through a low transverse axillary incison (1.0 cm in size) lateral to the pectoralis major. During the dissection, we identified sentinel nodes by following blue-stained lymphatic duct directly into blue-stained lymph nodes. We compared the value of two methods for identification of ESNB using blue dye only or a combination of blue dye and radioactive tracer.
Results
The mean number of sentinel nodes was 1.27 (range, 1-4). The identification rate and false negative rate of the sentinel node were 94.3% (132/140) and 6.9% (3/43), respectively. We compared ESNB with using blue dye only (n=77) vs. a combination of blue dye and radioactive tracer (n=63). Sentinel lymph node identification rate were 90.9% (70/77) vs. 98.4% (62/63) (p=0.043).
Figures and Tables
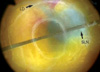
Figure 1
Endoscopic view of sentinel lymph node and draining lymph duct through Visiport. The arrow points to a dye-stained sentinel lymph node (SLN) and draining lymph duct (LD).


References
1. The Korean Breast Cancer Society. Nationwide Korean breast cancer data of 2004 using breast cancer registration program. J Breast Cancer. 2006. 9:151–161.
2. Krag DN, Weaver DL, Alex JC, Fairbank JT. Surgical resection and radiolocalization of the sentinel node in breast cancer using a gamma probe. Surg Oncol. 1993. 2:335–339.
3. Giuliano AE, Kirgan DM, Guenther JM, Morton DL. Lymphatic mapping and sentinel lymphadenectomy for breast cancer. Ann Surg. 1994. 220:391–398.

4. Kim T, Giuliano AE, Lyman GH. Lymphatic mapping and sentinel lymph node biopsy in early-stage breast carcinoma: a metaanalysis. Cancer. 2006. 106:4–16.
5. Kompatscher P. Endoscopic capsulotomy of capsular contracture after breast augmentation: a very challenging therapeutic approach. Plast Reconstr Surg. 1992. 90:1125–1126.
6. Tamaki Y, Tsukamoto F, Miyoshi Y, Tanji Y, Taguchi T, Noguchi S. Overview: video-assisted breast surgery. Biomed Pharmacother. 2002. 56:Suppl 1. 187s–191s.
7. Giuliano AE, Haigh PI, Brennan MB, Hansen NM, Kelley MC, Ye W, et al. Prospective observation study of sentinel lymphadenectomy without further axillary dissection in patients with sentinel node-negative breast cancer. J Clin Oncol. 2000. 188:2553–2559.
8. Schrenk P, Rieger R, Shamiyeh A, Wayand W. Morbidity following sentinel lymph node biopsy versus axillary lymph node dissection for patients with breast carcinoma. Cancer. 2000. 88:608–614.
9. McMasters KM, Tuttle TM, Carlson DJ, Brown CM, Noyes RD, Glaser RL, et al. Sentinel lymph node biopsy for breast cancer: a suitable alternative to routine axillary dissection in multi-institutional practice when optimal technique is used. J Clin Oncol. 2000. 18:2560–2566.
10. Friedlander LD, Sundin J, Bakshandeh N. Endoscopic mastectomy and breast reconstruction: endoscopic breast surgery. Aesthetic Plast Surg. 1995. 19:27–29.
11. Yamagata M, Iwai S. Endoscopic treatment for breast cancer. J Jpn Soc Endosc Surg. 1997. 2:272–277.
12. Tamaki Y, Sakita I, Miyoshi Y, Sekimoto M, Takiguchi S, Monden M, et al. Transareolar endoscopy-assisted partial mastectomy. Surg Laparosc Endosc Percutan Tech. 2001. 11:356–362.
13. Hinton CP, Doyle PJ, Blamey RW, Davies CJ, Holliday HW, Elston CW. Subcutaneous mastectomy for primary operable breast cancer. Br J Surg. 1984. 71:469–472.
14. Palmer BV, Mannur KR, Ross WB. Subcutaneous mastectomy with immediate reconstruction as treatment for early breast cancer. Br J Surg. 1992. 79:1309–1311.
15. Sawai K, Nakajima H, Mizuta N, Sakaguchi K, Hachimine T. Minimally invasive surgery for breast cancer. Gan To Kagaku Ryoho. 2001. 28:1063–1070.
16. Suzanne FY, Finkeltin FA, Bournazeau JA, Lemery DJ, Emering CM. A new, non traumatic technique about axillary lymphadenectomy using fat and lymph nodes suction aspiration. A study of thirty cases. Breast Cancer Res Treat. 1993. 27:188.
17. Salvat J, Knopf JF, Ayoubi JM, Slamani L, Vincent-Genod A, Guilbert M, et al. Endoscopic exploration and lymph node sampling of the axilla. Preliminary findings of a randomized pilot study comparing clinical and anatomo-pathologic results of endoscopic axillary lymph node sampling with traditional surgical treatment. Eur J Obstet Gynecol Reprod Biol. 1996. 70:165–173.
18. Kamprath S, Bechler J, Kühne-Heid R, Krause N, Schneider A. Endoscopic axillary lymphadenectomy without prior liposuction. Development of a technique and initial experience. Surg Endosc. 1999. 13:1226–1229.
19. Kuehn T, Santjohanser C, Grab D, Klauss W, Koretz K, Kreienberg R. Endoscopic axillary surgery in breast cancer. Br J Surg. 2001. 88:698–703.
20. Tsangaris TN, Trad K, Brody FJ, Jacobs LK, Tsangaris NT, Sackier JM. Endoscopic axillary exploration and sentinel lymphadenectomy. Surg Endosc. 1999. 13:43–47.
21. Kühn T, Santjohanser C, Koretz K, Böhm W, Kreienberg R. Axilloscopy and endoscopic sentinel node detection in breast cancer patients. Surg Endosc. 2000. 14:573–577.
22. Lee EK, Park YL, Pae WK. Endoscopic sentinel node biopsy. J Korean Breast Cancer Soc. 2003. 6:174–179.
 XML Download
XML Download