

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Breast cancer is the most common cancer among women in South Korea. A total of 11,275 women were newly diagnosed as having breast cancer in 2006 and the age-standardized incidence rate per 100,000 was 35.5.(1) Treatment for this common malignancy is a significant economic burden, for example, 190 billion won was paid for treating breast cancer by the Korean National Health Insurance in 2007.(2) Because the prognosis of breast cancer depends on the stage of the disease at presentation, adjuvant treatment that focuses on preventing recurrence of breast cancer has been an important treatment strategy for disease management and also for improving the patients' quality of life.
For women with early breast cancer, 5 yr' treatment with tamoxifen has been shown to reduce the risk of breast cancer recurrence by approximately 50% and the risk of death by approximately 25% compared with those receiving no hormonal therapy.(3) However, treatment with tamoxifen is associated with serious safety concerns including venous thromboembolism and endometrial cancer.(4) Anastrozole and Letrozole are the third generation aromatase inhibitors, and they have been demonstrated to be more effective than tamoxifen as the first-line treatment for early breast cancer for improving disease-free survival (DFS) when these drugs are administrated to women with post-menopausal hormone receptor positive breast cancer. The Arimidex, Tamoxifen Alone or in Combination (ATAC) trial and the Breast International Group (BIG) 1-98 trial are multinational, randomized clinical trials that compared 5 yr of monotherapy with an aromatase inhibitor (anastrozole and Letrozole, respectively) versus that with tamoxifen. Anastrozole has shown more favorable DFS (hazard ratio [HR], 0.83; 95% confidence interval [CI], 0.73-0.94; p=0.005) and a longer time to recurrence (HR, 0.74; 95% CI, 0.64-0.87; p=0.0002) versus tamoxifen on the completed treatment analysis of the ATAC trial, which was performed in postmenopausal women with early breast cancer.(5) Anastrozole was also associated with a more favorable safety profile versus tamoxifen, including a significantly lower incidence of endometrial cancer and thromboembolic events. These results confirmed the previously reported findings that were obtained at a median 47 months follow-up.(6) In the primary core analysis of the BIG 1-98 trial at a median follow-up of 25.8 months, letrozole significantly improved the DFS by 19% (HR, 0.81; 95% CI, 0.70-0.93; p=0.003), and it reduced the risk of breast cancer recurrence by 28% (HR, 0.72; 95% CI, 0.61-0.86; p=0.003).(7) Compared with the tamoxifen patients, the letrozole patients had lower risks of endometrial cancer and thromboembolism.(7) This superior efficacy for breast cancer recurrence was maintained, as was shown on the further follow-up results.(8,9) Although aromatase inhibitors have been reported to have a greater risk of cardiac events and fractures than tamoxifen,(5-9) they are effective and well-tolerated alternatives to tamoxifen for adjuvant treatment of postmenopausal women with hormone receptor positive breast cancer. However, the higher cost of aromatase inhibitors, against a background of increasing fiscal constraints on healthcare budgets, could limit the availability of this new treatment.
Economic evaluation is an analysis that compares a technology's cost and effectiveness in a real world setting and the result is shown as a cost-effectiveness ratio.(10) To be cost-effective, a new technology should generate more health gains for the patients than it displaces as a result of any additional cost imposed on the system (opportunity cost). This trade-off is assessed by comparing the incremental cost per final health outcome, which is usually presented as the quality-adjusted life years (QALY) gained. Within a given patient population it is possible to estimate the mean cost-effectiveness of an intervention compared with the relevant comparators. However, the 'average' cost-effectiveness can mask important sources of heterogeneity that may be reflected in the decision making by offering positive or negative guidance for patients with particular characteristics. For the patients with breast cancer, the population can be segmented by the nodal status, which is one of the prognostic factors for the risk of recurrence. When the cost-effectiveness of adjuvant therapies for treating early breast cancer is assessed, the results of the subgroup analysis can contradict the results for the overall population.
The purpose of this study is to address the cost-effectiveness of 2 aromatase inhibitors, anastrozole and letrozole, versus tamoxifen when they are used to treat women with postmenopausal hormone receptor positive early breast cancer in the Korean context. Moreover, this study aims to find the most reasonable treatment option among the node positive patients and node negative patients, when the population is stratified by the risk of recurrence.
METHODS
Overview
Markov model is an analytic framework that enables modeling the progression of chronic disease such as cancer over long periods of time. Markov model is based on a series of 'states' that describe each step of the disease progression, and patients can occupy these states at a given point in time. The time duration during which the average patients stay in the states of the model will be used to calculate the expected cost and outcomes. The likelihood of moving between the states in the model is determined by a set of transition probabilities.(11) A health state in the model has values including a 'cost' and an 'effectiveness'or 'utility' value associated with it. These values given to each Markov state are weighted by the time a patient spends in that state.
In our model, the expected lifetime costs and health outcomes, including life years (LYs) and QALYs, were calculated for each treatment. Then the lifetime costs and health outcomes were combined to estimate the incremental cost-effectiveness ratio (ICER) of aromatase inhibitors versus tamoxifen. The analysis was conducted from a societal perspective and all the cost estimates were adjusted to the first half year of 2009. Both the costs and QALYs were discounted with a 5% rate to convert the future values incurred during the analytic timeframe into present values.
Because there have been no head-to-head clinical trials between anastrozole and letrozole whose long-term follow-up data is available, this study used indirect comparison with applying tamoxifen as a common comparator to compare the cost-effectiveness between anastrozole and letrozole. When applied to the same model, we could estimate the ICER of anastrozole vs. tamoxifen and that of letrozole vs. tamoxifen, respectively. After estimating the ICERs of the overall population, a sub-group analysis was conducted with stratification by the nodal status.
Structure of the economic model and the assumptions
The characteristics of the patients entering this model followed the patient characteristics of the ATAC and BIG 1-98 trials. They were assumed to be 50 yr of age and to have initiated adjuvant therapy with aromatase inhibitors or tamoxifen after completing breast cancer surgery and chemotherapy when needed. The adjuvant treatment was continued for 5 yr or until the occurrence of a breast cancer event (contralateral breast cancer, locoregional recurrence or distant recurrence). The patients were assumed to be at risk for breast cancer events for 15 yr after the breast cancer diagnosis or any breast cancer event. Mortality and the health-related quality of life were assumed to be influenced by the breast cancer events and the treatment related adverse events.
The health states of this model were defined based on the disease stage of breast cancer, and the health states were described according to 6 states; disease-free, disease-free with treatment related adverse events, contralateral breast cancer, locoregional recurrence, distant recurrence and death. The disease-free patients were at risk for 3 types of recurrence (contralateral breast cancer, locoregional or distant recurrence) and the patients with contralateral recurrence were at risk for locoregional or distant recurrence (Figure 1). Adjuvant treatment was assumed to reduce the risk of these recurrences, but to increase or decrease the risk of adverse events, including endometrial cancer, thromboembolic events, cardiac events or fractures. Regarding the 'carry-over effects' of adjuvant treatment, the duration of benefits was assumed to remain even after treatment had stopped based on the results from the Early Breast Cancer Trialists' Collaborative Group (EBCTCG) meta-analysis for tamoxifen.(12) We assumed 5-yr of carry-over for aromatase inhibitors. The transition probabilities between states were acquired as annual probabilities and all the outcomes were evaluated over a 35-yr timeframe beginning with the initiation of adjuvant therapy and approximating a lifetime projection. The model was programmed using TreeAge Pro™ 2009 (TreeAge Software Inc., Williamstown, USA), which is decision analysis software.
Model estimation
Probabilities of breast cancer events
The annual probabilities regarding breast cancer recurrence were estimated using published data, including the EBCTCG meta-analysis, the ATAC trial and the BIG 1-98 trial. For the patients receiving tamoxifen, the annual probabilities of the first breast cancer events in the years 1-5 of this model were obtained from the ATAC and BIG 1-98 trials. For extrapolation after year 6, this annual probability of recurrence was adjusted using the annual trend of recurrence presented from the EBCTCG metaanalysis, which reported the annual probability of recurrence with tamoxifen treatment for 15 yr. For anastrozole and letrozole, the probabilities of first breast cancer events were obtained by multiplying the probabilities for tamoxifen by the HR for breast cancer recurrence from the ATAC trial(5,6,13) and the BIG 1-98 trial,(7,8) respectively (Table 1). The proportions of the first breast cancer events, which would be contralateral tumor, locoregional recurrence and distant recurrence, were based on the distribution of first events among the Korean breast cancer women by applying Yang's study (5%, 17%, and 78%, respectively).(14)
The annual probabilities of recurrence following contralateral tumor were estimated from the 1998 EBCTCG meta-analysis.(3) The annual probabilities of distant metastases among the patients with locoregional recurrence were estimated by pooling the eight studies that reported such data.(15-22) It was assumed that the relative frequencies of locoregional recurrence and distant metastases following contralateral tumor would be the same as those of the disease-free patients according to the previous cost-effectiveness analysis studies (Table 2).(23,24)
When subgroup analysis was performed, different HR values by the nodal status were used. For the node negative group, the HR of anastrozole vs. tamoxifen for first breast cancer events was 0.69 (95% CI, 0.43-0.95),(12) while the HR of letrozole vs. tamoxifen was 0.88 (95% CI, 0.70-1.10)(8) for this subgroup. For the node positive group, the HR of anastrozole vs. tamoxifen for first breast cancer was 0.87 (95% CI, 0.67-1.07)(12) and the HR of letrozole vs. tamoxifen was 0.77 (95% CI, 0.64-0.92) (Table 3).(8)
Probabilities of adverse events
Five treatment-related adverse events (endometrial cancer, thromboembolism, ischemic heart disease, hip fracture and other fracture) were considered in this model according to the ATAC and BIG 1-98 trials.(5-9) When these adverse events were selected, the clinical significance to mortality, the frequency of the adverse events during the hormonal treatment and their acceptance in both the ATAC and BIG 1-98 trials were considered. The annual probabilities of these events among the general Korean female population were estimated from previous studies that reported this data. The estimates of the relative risk (RR) of adverse events for tamoxifen versus no endocrine therapy were based on the data from the National Surgical Adjuvant Breast and Bowel Project (NSABP) P-1 study.(25) The estimates of the RR of adverse events for aromatase inhibitors versus tamoxifen were based on the published data on the number of patients with adverse events reported in the ATAC or BIG 1-98 trial, respectively (Table 4).
Probabilities of death
The age-specific annual probabilities of death for women without distant metastases or adverse events were obtained from the age-specific mortality rates for the Korean female population,(31) with excluding the mortality rates due to breast cancer and the adverse events defined in this study (Table 5).
The annual probability of death among the women with locoregional recurrence was estimated to be 17.4% based on the data from Stokes.(32) The annual probability of death due to distant recurrence was obtained based on the clinical trial data for metastatic breast cancer patients.(33)
Because the probabilities of death from adverse events, including endometrial cancer, thromboembolism, ischemic heart disease and fractures, for the Korean female population have not been reported, the data reported by other countries were used. Disease specific mortality due to endometrial cancer was reported to have an additive mortality increase of 2.5%.(34) Thromboembolism was reported to increase the risk of mortality, and this varied by 1-33.4% depending on the data,(35,36) and the data was pooled to an estimated 12.3% of additive increase of mortality. The RR of death for ischemic heart disease was reported to be 4.0.(37) The RR of death for hip fracture was estimated to be 3.0,(38) while the other fractures have the same risk of death as that for the general population.
Costs of adjuvant hormonal therapy
The costs of adjuvant treatment with tamoxifen, anastrozole and letrozole included the drug costs, pharmacy fees and the costs of diagnosing the hormone receptor status. Drug costs were based on the 2009 pharmaceutical prices that were weighted by the prescription volume, which was issued by the Korean Health Insurance Review and Assessment Service (HIRA) in the first half year of 2009 (Table 6).
Costs of breast cancer events
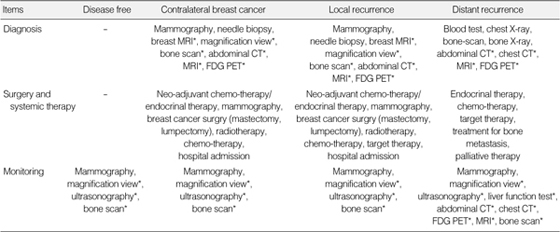
The costs that occur in each breast cancer state, including disease-free, contralateral breast cancer, locoregional breast cancer and distant breast cancer, are composed of the cost of the diagnosis, the treatment cost and the monitoring cost. It is assumed that the patients follow the Clinical Practice Guideline for Breast Cancer.(39) The total use of resources was measured by multiplying the unit cost of each resource item by the frequency of resource use by applying micro-costing methods. When each resource item was included, the standard guideline for breast cancer diagnosis and treatment(39) was referred to (Appendix). The cost of visiting the doctor and the transportation cost were included in each diagnosis and treatment. The unit cost of the each resource item was obtained from the list of fee schedule from the HIRA as of 2009. The estimated total costs by the defined health states are shown in Table 7.
Costs of the adverse events and the non-health care costs
The average cost of each adverse event related to adjuvant treatment was extracted from the National Health Insurance Statistical Yearbook (NHISY), which is where the annual payment of the NHI by the disease category was reported.(2) The annual average treatment costs for endometrial cancer, thromboembolic events, ischemic heart disease, hip fracture and other fractures were estimated based on payment of the NHI. Because the newest version of the NHISY had the statistics as of 2007, we adjusted these costs to as of 2009 using the Consumer Price Index.(40) According to the ATAC and BIG 1-98 trials, the frequency of each adverse event varied with the adjuvant treatments. To estimate the average cost for treating adverse events by the adjuvant treatment, the frequency of each adverse events reported in the ATAC and BIG 1-98 trials was used as weight.
The costs for transportation and care-givers were included as non-health care costs. To estimate the unit costs for these items, the data reported from the Korea National Health and Nutrition Examination Survey (KNHNES) 2005 was applied. All the costs were adjusted for 2009. The data of the KNHNES 2005 was multiplied by the annual Consumer Price Indexes from 2005 to 2009. The average annual rate of inflation was estimated as 3.3%.
Sensitivity analyses
When conducting the deterministic sensitivity analysis, the key model parameters, including probabilities, cost and relative risks, were varied from 50% to 150% of the base-case values. The results for the model timeframe of 25 yr and a drug price reduction by 10% were also generated. The role of a discount rate was also examined in the sensitivity analysis, with the range of 3% to 7%.
RESULTS
Base-case analysis
Anastrozole and letrozole both showed additional health benefits versus tamoxifen and they were more costly than tamoxifen as well. In the first model, which analyzed anastrozole versus tamoxifen, the discounted QALY were shown as 11.36 and 11.13, respectively, while the discounted lifetime cost of anastrozole and tamoxifen were Korean Won (KRW) 14,445,950 and KRW 9,260,723, respectively. In the second model where letrozole and tamoxifen were analyzed, the discounted QALY were shown as 11.37 and 11.08, respectively, while the discounted lifetime cost of letrozole and tamoxifen were KRW 15,404,289 and KRW 9,419,457, respectively. These increases in the expected cost and health outcome were combined and this produced an incremental cost-effectiveness ratio (ICER). When the ICERs of anastrozole and letrozole were compared in the overall population, it was not confirmative to decide which treatment was superior because their cost per QALY was similar to each other. However, when subgroup analysis was conducted, it became clear that anastrozole was more cost-effective than letrozole for the node negative group and letrozole was more cost-effective than anastrozole for the node positive group (Table 8).
Sensitivity analyses
Because the costs of adjuvant treatment were a major part of the total treatment costs for early breast cancer, cost-effectiveness was sensitive to the reduction of price of aromatase inhibitors. Also, cost-effectiveness was relatively sensitive to the probability of death due to distant recurrence, the costs of death from breast cancer, the RR of hip fracture for aromatase inhibitors versus tamoxifen and the discount rate. In both models that analyzed the cost-effectiveness of anastrozole (Model 1) and letrozole (Model 2), these variables changed the cost-effectiveness ratio into lower or higher ones, yet no parameters made the ICER a negative value, and so the result was that aromatase inhibitors are inferior to tamoxifen (Figure 2). Moreover, the narrow range of variation for the ICER (presented within 2.5 million won) showed that our base-case results are robust.
DISCUSSION
The cost-effectiveness analysis in this study assessed the benefits of aromatase inhibitors versus tamoxifen as primary adjuvant therapy for postmenopausal women with hormone receptor positive early breast cancer. The patients were stratified by their nodal status at the time of diagnosis and the cost-effectiveness of each adjuvant treatment was estimated for the node negative group and the node positive group, respectively. A Markov model was applied using the data from a variety of sources of published data. Transition probabilities between the defined states, the lifetime costs related to breast cancer treatments and QALYs as the final health outcome were estimated. The results of this study showed that the aromatase inhibitors, anastrozole and letrozole, have more benefits than tamoxifen. The benefits of anastrozole would be provided at an incremental cost of KRW 22,461,689 per QALY gained, while the benefits of letrozole would be provided at an incremental cost of KRW 21,004,142 per QALY gained. When the population was stratified by the nodal status, anastrozole turned out the most cost-effective treatment option among the adjuvant hormonal therapies with showing an incremental cost of KRW 19,717,770 per QALY gained in the node negative group, while letrozole turned out the most cost-effective with incurring an incremental cost of KRW 8,150,512 per QALY gained in the node positive group.
There are no explicit guidelines by the Korean government specifying a threshold value of cost per QALY gained that can be used to determine whether a therapy provides good value for the money. In the previous studies in the US, $US 50,000 per QALY was quoted as a threshold to define cost-effectiveness (KRW 57,500,000 per QALY at the exchange rate as of January 2010).(42,43) Other Canadian studies have suggested that therapies with a cost per QALY gained within $Can 28,000 should be considered as cost-effective (KRW 30,500,000 per QALY). In this context, the incremental cost-effectiveness ratios of this study can be accepted in the Korean context as well.
The distinguishing feature of this study appeared on the subgroup analysis. Several studies have conducted a cost-effectiveness analysis for aromatase inhibitors versus tamoxifen for patients with postmenopausal hormone receptor positive early breast cancer,(42-46) but none of them were implemented in Asian counties nor did the studies conduct a subgroup analysis. When anastrozole and letrozole were compared in the overall population, their difference in cost per QALY was not big enough to conclude that any of them was superior to the other. However, after the population was divided by the nodal status, it became clear to suggest a more cost-effective alternative for each subgroup. Moreover, letrozole for the node negative group was inferior to tamoxifen in terms of the incremental cost per QALY gained, which presented as a negative ICER.
Anastrozole and letrozole were introduced around the same time in Korea with similar prices. They maintained similar prices in the past, but recently their prices have largely been reduced through price re-evaluation, and the introduction of generics has made anastrozole have a lower price than letrozole by about 10%. We assessed the cost-effectiveness again under the assumption that anastrozole and letrozole have same prices with an additional price reduction of letrozole by 10%. When their prices were the same, the cost per QALY of letrozole was significantly lowered from KRW 21,004,142 to KRW 18,204,570 per QALY gained and this was even more favorable than the base-case results of anastrozole, whose cost per QALY gained was KRW 22,461,689. The costs of adjuvant hormonal treatment account for the majority of the lifetime treatment costs for early breast cancer, so the slight change in the drug price influenced the overall results.
The lack of observed survival benefits as well as long-term effects on the benefits and toxicities creates challenges to accurately forecast the cost-effectiveness ratios. This is a common challenge with modeling and it is generally resolved with appropriate assumptions and extrapolations. The assumptions can be supported by reliable, accepted literature or similar sources. In this study, it was assumed that the relative frequencies of locoregional recurrence and distant metastases following contralateral tumor would be the same as that in the disease-free patients according to the previous cost-effectiveness analysis studies.(23,24) There has been no literature that has reported the long-term recurrence rate after the occurrence of contralateral breast cancer.
Indirect cost was considered in this study using the productivity approach to estimate the cost of pre-mature death due to breast cancer. The loss of productivity during hospitalization or a doctor visit was also considered. However, the population of this study was post-menopausal women aged 50 and they usually do not participate in economic activities. Because the estimated loss of productivity in terms of lost income among Korean women aged 50 or older was very small, we did not include these costs regarding productivity.
To obtain the utility value of the breast cancer states among Korean women, this study inevitably used published data from foreign countries. The health-related quality of life and utility of Korean breast cancer women have been reported in several studies, yet these studies could not be applied to our study. The Korea Institute for Health and Social Affairs suggested the utilities of the major chronic disease in Korea including breast cancer, but the utilities of each breast cancer state were not reported.(47) The study of Ahn et al.(48) measured the health-related quality of life for a disease free state after breast surgery with focusing on the type of adjuvant treatment or the type of surgery, but the results were not applicable for this study. When conducting the cost-effectiveness analysis, it has been accepted to quote foreign data for utility or some epidemiological data, but further research on this area should be conducted to obtain more accurate estimates.
There are two methods for the economic evaluation of pharmaceuticals. One is to use secondary data source, which is the method used in this study, and the other is to conduct randomized controlled trials (RCTs) or pragmatic controlled trials (PCTs) to achieve data on treatment effectiveness and cost. The methods to conduct RCT or PCT, however, are not free from caveat. They need considerable resources like time, money and work force. They have a pre-defined setting such as inclusion criteria of patients and intervention methods, so their external validity can be challenged. The long-term follow-up results from RCT or PCT can hardly be achieved. Additionally, when we use the local data source, its internal validity should be considered. For those reasons, using accepted literatures as secondary data source has sometimes more benefits than conducting RCT or PCT.
The progress in the methodology of economic evaluation, therefore, has been focused on how to reduce the bias from using different sources of data and how to appropriately extrapolate lifetime effectiveness and costs. To use relative risk or hazard ratio with baseline characteristics being controlled for is one of the good practices for the economic modeling using secondary data. In this study, we used secondary data source to estimate the effectiveness of each treatment, but we estimated the treatment cost in Korean context using the micro-costing method. We suggest that the results of this study could be applied to Korean patients.
CONCLUSION
The findings of this study were summarized as follows. First, anastrozole and letrozole were both cost-effective treatments compared to tamoxifen. Second, when anastrozole and letrozole were compared indirectly in the overall population, their cost-effectiveness ratios were too similar to decide which treatment was superior to the other. Third, when the population was divided by the nodal status, it became clear that anastrozole was more cost-effective than letrozole in the node negative group and letrozole was more cost-effective than anastrozole in the node positive group. The decision makers of health policy need to be careful when generalizing these cost-effectiveness results to the overall population. The subgroup results in this context can be used to more efficiently allocate resources and to enhance the value of the decisions that are made on health policy in Korea.










 XML Download
XML Download