

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Breast cancer, the most common malignancy in women, is characterized by a distinct pattern of metastases involving regional lymph nodes, lung, bone, and liver. Even though early stage breast cancers are not life threatening, metastatic breast cancer is responsible for the majority of cancer-related deaths. Metastasis is the result of several sequential steps and represents a highly organized, nonrandom, and organ-selective process.(1) Chemokines and their respective receptors regulate chemotaxis and the transendothelial migration of leukocytes during immune and inflammatory reactions.(2) Although different kinds of cancer cells express different chemokine receptors, the most common expressed on human cancer cells is the CXC chemokine receptor CXCR4, which has been found in at least 23 different types of human cancer, including those of epithelial, mesenchymal, and hematopoietic origin.(3) Expression of CXCR4 has been demonstrated in breast cancer, melanoma, some leukemias,(4) prostate and ovarian cancers,(5) B-cell lymphomas,(6) primary pancreatic cancer cell lines,(7) renal cell carcinoma(8) and bladder cancer.(9) CXCR4 is activated by its only known ligand, stromal cell-derived factor-1α (SDF-1α). Activation of CXCR4 induces signal transduction pathways in cancer cells that are important in the cancer metastasis procedure with involvement in cytoskeletal rearrangement, actin polymerization,(4) pseudopodia formation, firm adhesion to endothelial cells, directional migration and proliferation.(10) Dewan et al.(11) found that the SDF-1 receptor CXCR4 was over-expressed in human breast cancer tissues and was linked to the nodal spread of breast cancer. Also, CXCR4-expressing breast cancer cells aggressively metastasized in secondary organs. Sun et al.(12) found that SDF-1α was expressed in all lymph cells in lymph nodes, including metastatic and non-metastatic, suggesting that the expression of SDF-1α in lymph nodes probably participates in CXCR4 signal-directed migration of breast cancer cells into the lymph system. SDF-1 was specifically expressed in malignant cell types including breast cancers, pancreatic cancers, glioblastomas and oral squamous cell carcinoma.(6,13) Neutralization of SDF-1/CXCR4 interaction significantly inhibits the metastasis of breast cancer cells to distant organs.(11) Helbig et al.(14) found that studies using mouse models of breast cancer and specimens from human tumors had emphasized the importance of the tumor microenvironment in controlling the SDF-1/CXCR4 signaling pathway.
The primary objectives of this study were to investigate the correlation between CXCR4 and axillary lymph node metastasis and to clarify the interaction of CXCR4 in primary tumor cells and SDF-1α in metastatic lymph nodes. An analysis of the correlation between CXCR4, SDF-1α, and clinicopathologic features was also performed.
METHODS
Patients and tissue specimens
Forty-four invasive ductal carcinomas, which were surgically resected in the Department of Surgery and diagnosed in the Department of Pathology at the Catholic University Daejeon St. Mary's Hospital from January 2000 through January 2009, were obtained. Ipsilateral axillary lymph node dissection was performed in all cases.
Clinicopathologic parameters were evaluated, including age at initial diagnosis, tumor size, nuclear grade, histologic grade, lymph node metastasis and pathologic node (pN) stage pN0 to pN3. The histologic grade was assessed according to a modified Bloom-Richardson-Scarff grading system.
Construction of tissue microarrays (TMAs)
Hematoxylin-eosin stained slides were reviewed for each case and areas of interest were marked on each slide. The arrays were constructed using a 5 mm punch on a Bee-Cher arrayer. Corresponding regions were circled on the "donor" paraffin block using a marker pen. Samples were then arrayed on a "recipient" blank block. A total of 19 samples were available for 1 array.
Immunohistochemistry
Immunohistochemical staining for CXCR4 (Abcam, Cambridge, UK), SDF-1α (Abcam, Cambridge, UK), estrogen receptor (ER) (Immunotech, Paris, France), progesterone receptor (PR) (Immunotech, Paris, France) and HER2 (DAKO, Copenhagen, Denmark) were performed on TMA sections. Briefly, 4 µm thick sections were cut from paraffin blocks. The wax was removed from the paraffin sections using xylen, followed by rehydration through a series of graded alcohols, placement in 10 mL of citrate buffer, and submitted for heat retrieval using a vapor lock for 30 min. After heating, the slides were allowed to cool to room temperature then briefly washed with tris-buffered saline (DAKO, Copenhagen, Denmark). Then the slides were immersed in a 3% H2O2 solution to block endogenous peroxidase activity, and incubated for 1 hr with primary antibodies for ER, PR and HER2. Primary antibodies for CXCR4 and SDF-1α were incubated overnight at 4℃. After incubation, slides were stained with peroxidase-labeled streptavidin-biotin complex (Zymed, San Francisco, USA) and counterstained with Mayer's hematoxylin.
CXCR4 was considered to be positive when breast cancer cells showed the cytoplasm, the nucleus, and/or the complete membrane as a brown color. The staining pattern of tumors for CXCR4 was defined as cytoplasmic expression, nuclear expression or membranous expression using the criteria in Table 1.(15,16)
SDF-1α was considered to be positive if more than moderate cytoplasmic staining of malignant cells, but not nuclei, was observed. If the sum of the proportion score and the intensity score(17) was more than 3, ER and PR were considered to be positive. Only cells with a membranous staining score 3 were considered positive for HER2.
We performed immunohistochemical staining for both ER and PR three times because of a low percentage for positivity.
Statistical analysis
The SPSS for Window 12 software package (SPSS Inc., Chicago, USA) was used for statistical analysis.
The tumor size, nuclear grade, histologic grade, and pathology of lymph nodes (pN) of the clinicopathologic features were analyzed using the chi-square test. Fisher's exact test was evaluated used for the remaining clinicopathologic features. The intergroup difference in CXCR4 and tumor size was evaluated by Student's t-test. Pearson's r correlation was also used to estimate correlation coefficients between hormone receptors and histologic or nuclear grade, between ER expression and HER2 expression, and between age and CXCR4 expression. p-values of less than 0.05 were considered statistically significant.
RESULTS
Interaction of CXCR4 and SDF-1α in breast cancer, lymph nodes, normal breast tissue, and clinicopathologic features
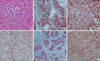
In total, 44 invasive ductal carcinomas were analyzed (Figure 1A). Patient age ranged from 28-77 yr with a mean age of 52 yr. CXCR4 expression in breast cancer was negatively correlated with increased age (≥52 yr) (p=0.005), and positively correlated with a larger tumor size (p=0.043 analyzed using the Fisher's exact test and p=0.020 evaluated by Student's t-test) and PR expression (p=0.027). CXCR4 expression in breast cancer was not correlated with metastatic lymph nodes (p=0.079) nor SDF-1α expression in metastatic lymph nodes (p=0.062) (Tables 2, 3).
The staining patterns of CXCR4 in breast cancer varied as follows: no staining (19 cases), nuclear expression (15 cases, Figure 1B), cytoplasmic expression (9 cases, Figure 1C) and membranous expression (1 case, Figure 1D).
CXCR4 nuclear expression in breast cancer appeared more frequently in lymph node-positive tumors (55.6%, p=0.023) than in lymph node-negative tumors (19.2%). CXCR4 cytoplasmic expression in breast cancer was not correlated with lymph node metastasis (Table 4). CXCR4 expression was absent or minor in normal breast epithelia.
Breast cancer cells were stained by SDF-1α in primary breast cancers (Figure 1E) and in the lymph nodes (Figure 1F). Lymphoid cells were also stained by SDF-1α in primary breast cancers and in the lymph nodes. SDF-1α expression was negative in normal ductal and lobular cells. SDF-1α in breast cancer was not correlated with any clinicopathologic features (Table 2).
Correlation between hormone receptor (ER and PR) expression, and CXCR4 and SDF-1α
Coexpression of ER and PR was present in 10 breast cancers. ER positivity (Figure 2A) was not correlated with the expression of CXCR4 and SDF-1α in breast cancers. PR positivity (Figure 2B) was correlated with CXCR4 positivity in primary breast cancers (p=0.027) and not correlated with SDF-1α in metastatic lymph nodes (Table 2).
Correlation between ER or PR expression, and histologic grade or nuclear grade, and between ER expression and HER2 expression
ER or PR expression was negatively correlated with histologic grade (p=0.017, r=0.428 and p=0.017, r=0.391). ER or PR expression was negatively correlated with nuclear grade (p=0.029, r=0.397 and p=0.014, r=0.392). ER expression trended toward a negative correlation with HER2 expression (p=0.61, r=0.282).
DISCUSSION
The mechanism of metastasis to lymph nodes is not well understood. Recent studies have shown that CXCR4, CCR7, and c-MET are involved in directing tumor cells to lymph nodes.(7) Activation of SDF-1α/CXCR4 increases secretion of MMP2 and MMP9. These signaling events result in changes in cellular motility and invasive and adhesive properties in breast cancer cells. Collectively, these events may lead tumor cells to metastasize to lymph nodes. Experimental studies have suggested that several tumor types metastasize to distant organs, such as the lungs and bones, via the CXCR4-mediated signaling pathway.(3)
Sun et al.(12) found that SDF-1α is involved in CXCR4-stimulated directed metastasis of cancer cells. CXCR4 protein expression increases with tumor aggressiveness, and levels of SDF-1 are higher in metastatic lesions than in primary tumor sites. Tumor invasion and metastasis involve complex procedures in which the invasion of tumor cells and passage through the basement membrane, fibroblast monolayers and endothelial cells are regarded as key processes before the tumor cells migrate to target organs. Directed migration of tumor cells stimulated by activation of CXCR4 is dependent on an SDF-1α gradient.(9) It has been reported that 100-1,000 ng/mL of SDF-1α is an optimal concentration to stimulate the migration of monocytes, lymphocytes, endothelial cells, and tumor cells. By using time-lapse monitoring of the locomotion of individual cells, it was shown that SDF-1α accelerates the motility of several different kinds of human tumor cells, including breast cancer, rhabdomyosarcoma and small lung cancer cell lines.(10) The mechanisms by which SDF-1α effects tumor cell motility include changes/rearrangement of the cytoskeletal proteins, augmentation of the number and thickness of F-actin bundles, and calcium flux.(11) Based on a Matrigel invasion model, SDF-1α is probably also involved in cancer cell growth and survival, in addition to stimulating cancer cell migration. Because cancer cells experience little growth when deprived of a blood supply during metastasis to distant sites, SDF-1α probably helps in the survival and spread of cancer cells by stimulating their proliferation. CXCR4/SDF-1α participates in vivo and directs migration in vitro.
Tumor cell metastasis may be correlated with attraction of SDF-1α to the metastatic organ. Our results showed that CXCR4 expression in breast cancers tended toward a positive correlation with SDF-1α expression in lymph nodes-positive tumors, even though the correlation was not statistically significant (p=0.062).
A high level of cytoplasmic CXCR4 expression occurs more commonly, but not significantly, in lymph node-positive tumors.(15,18) The results of Woo et al.(19) showed that expression of CXCR4 in the cytoplasm is not associated with axillary lymphatic metastasis. CXCR4 is a membrane-bound G-protein-coupled receptor that can be internalized together with its ligand SDF-1 upon activation. Therefore, cytoplasmic reactivity, especially when co-expressed together with SDF-1, may reflect receptor internalization and, thus, a state of activation of CXCR4.(20) Predominantly nuclear CXCR4 staining was more likely to be statistically significant in lymph node-negative tumors.(15,18) Su et al.(21) reported that a high level of CXCR4 nuclear expression was not associated with lymph node involvement. Spano et al.(22) pointed out that in non-small cell lung carcinoma, CXCR4-positive nuclear staining might be associated with survival. They opined that the nuclear retention of CXCR4 decreases cell proliferation and metastasis by inhibiting the interaction with SDF-1α. Shim et al.(23) stated that SDF-1 induces both down-regulation of membranous CXCR4 expression and degradation of the internalized CXCR4 receptors via the lysosome pathway. These results suggest that a reduction in CXCR4 membrane staining in metastatic lymph nodes is associated with progression of breast cancer metastasis.
Our results showed that CXCR4 nuclear positivity is correlated with lymph node metastasis and that CXCR4 expression trended toward a positive correlation with metastatic lymph nodes (p=0.079). These results indicate that different patterns of CXCR4 expression in cells probably lead to differences in the biological behavior of the respective tumor cells. Evaluation of the expression patterns will help predict lymph node metastasis and clinical outcomes.
Woo et al.(19) found that neither cytoplasmic nor nuclear CXCR4 expression shows a significant correlation with other characteristics including age, tumor stage, node stage, tumor-node-metastasis (TNM) stage, histological grade, ER, PR, or HER2 status.
We found that the positivity of CXCR4 in breast cancer is negatively correlated with increased age (≥52 yr). Assuming a normal age distribution in breast cancer occurrance, the sample mean (52 yr) of observed ages is considered to be an estimate of the population mean. The p-value and the correlation coefficient (Pearson's r) for increased age (≥52 yr) and CXCR4 positivity were 0.005 and -0.445, respectively. These show an inverse relationship between increased age (≥52 yr) and CXCR4 positivity.
High-intensity immunohistochemical staining for CXCR4 was associated with large tumors in papillary thyroid carcinomas (p=0.02)(24) and CXCR4 was also expressed strongly in large tumors of non-small cell lung cancers (>3 cm, p=0.042).(25)
Woo et al.(19) found that among 105 breast cancers, 26 cases (24.8%) were classified as T1, 63 cases (60%) as T2 and 16 cases (15.2%) as T3. Nuclear and cytoplasmic CXCR4 were not correlated with tumor size. However, our results showed that a larger tumor size was correlated with CXCR4 expression.
Salvucci et al.(26) found an inverse correlation between cytoplasmic CXCR4 staining and ER positivity, and no correlation between either cytoplasmic or nuclear CXCR4 staining and PR positivity. A negative estrogen and a progesterone receptor status were significantly correlated with a high level of nuclear CXCR4 expression and with lymph node metastasis. Furthermore, there was a significant correlation between a high level of nuclear CXCR4 expression and lymph node metastasis and receptor negative estrogen and the progesterone status.(19) We found that CXCR4 was positively correlated with PR expression but wasn't with ER positivity.
Recently, the Breast Pathology Study Group of the Korean Society of Pathologist collected 1,198 breast carcinoma samples from seven university hospitals and performed ER staining with the three antibodies, 1D5, 6F11 and SP1. The ER positivity rates were 68.6% for SP1, 59.5% for 1D5 and 54.8% for 6F11.(27) In our study, the ER expression rate in breast cancers was 36.4% with the 1D5 estrogen receptor clone. Also, among the other 72 excised breast cancers without lymph node dissection, the ER expression rate was 35 cases (48.6%). In our study, negative ER or PR expression was correlated with a high histologic grade or high nuclear grade. These ER expression rates may be attributable to high histologic grade cancers, high nuclear grade cancers, different kinds of antibodies used, differences between the products of manufacturing companies, the duration of fixation, the buffer solutions used, tumor heterogeneity, or a small number of cases.
CONCLUSION
An evaluation of young age, large tumor size and PR expression helps predict lymph node metastasis and poor prognosis. Expression of CXCR4 nuclear positivity is correlated with a poor prognosis. A larger study is needed to verify these results and further study is needed to determine the clinical significance of SDF-1α/CXCR4 expression.





 XML Download
XML Download