

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Nonpalpable breast cancers have a better prognosis than palpable breast cancers, and a higher incidence of ductal carcinoma in situ (DCIS), a lower tumor stage, and a lower incidence of lymph node metastasis.(1-7) Currently, mammography has been used with clinical breast examination and breast self-examination for screening of breast cancer.
Mammography has been successfully used as a screening test for breast cancer over the past 20-30 yr, but has substantial limitations. Approximately 10-20% of palpable breast cancers are not visible on mammographic images, mainly due to insufficient contrast between normal and abnormal breast tissue.(8-10) Moreover, the sensitivity of mammography for the diagnosis of breast cancer is variable and known to be influenced by age, breast density, family history, and other factors.(11) False negative rates for mammographic breast cancer detection are higher in women with dense breast parenchyma, and the risks of subsequent breast cancer are also higher, particularly in women with a first-degree family history of breast cancer.(12-14)
Breast ultrasound (US) is widely used as a supplementary modality for evaluating mammographically detected abnormalities,(15-17) and as an effective screening modality for detecting occult breast cancers in mammographically determined dense breasts.(15, 17-21) A study by Stavros et al.(22) reported that US has a high sensitivity and negative predictive value for diagnosing breast cancer, i.e., 98.4% and 99.5%, respectively, and recent advances in US technology and transducer design permit greater spatial and contrast resolution. Therefore, we decided to investigate the correlation between breast US and clinical findings in patients with breast cancer. Specifically, this study was undertaken to evaluate US findings in palpable and nonpalpable breast cancers and to identify US features that differentiate these two cancer groups.
MATERIALS AND METHODS
1. Patients
This study was approved by the institutional review board for human investigation. We searched patients who underwent surgery for primary breast cancers at our cancer center from January 2002 to August 2004 using a computer data base system. The total number of patients that had undergone breast cancer surgery during this period was 370. Two hundred nineteen patients underwent modified radical mastectomy, 151 breast conservation therapy, and 309 axillary lymph node dissection. Of these 370 patients, 201 patients underwent breast US before surgery and 191 patients had an abnormal US finding, and these 191 patients were included in this study. All patients were female and ages ranged from 27 to 82 yr (mean, 48 yr).
Breast cancers were considered palpable if they were detected by physical examination by at least one physician before treatment.(6, 18) Patients at our institution are routinely examined by multiple experienced clinicians before treatment, i.e., radiologists, surgeons, medical oncologists, and plastic surgeons. If a lesion was detected by any physician, then it was scored as a palpable breast cancer. Nonpalpable cancers were identified using abnormal imaging study findings. One hundred twenty one of the 191 patients had palpable breast cancer and the remaining 70 patients, nonpalpable breast cancer. Of the 70 patients with nonpalpable breast cancer, 14 patients had nipple discharge and 3 patients had skin eczema. In total the 191 patients had 200 breast cancers, 167 of which were invasive carcinomas and 33 were DCIS cases. Nine patients had ipsilateral multiple breast cancers.
One hundred four of 191 patients obtained mammography and 99 patients were available for evaluation of mammography. The mammographic findings of these 99 patients were: mass in 38, mass with calcifications in 22, focal asymmetry in 10, architectural distortion in 1, calcifications only in 8, and no lesion in 20.
2. Evaluation points
In our institute, US is routinely performed as an initial examination for palpable masses in women younger than 35 yr, and for nonpalpable masses detected by mammography, to allow mass characterization. US is also performed to screen women with mammographically dense breasts. One hundred ninety one patients in this study underwent breast US to further evaluate; abnormal mammographic findings (n=73), to screen mammographically dense breasts (n=47), and those with symptoms but without specific mammographic abnormalities (n=10), and as an initial examination in young women (n=61).
All patients were examined using a Logiq9 unit (General Electronic Medical System, Milwaukee, USA) or a HDI 5000 unit (Advanced Technology Laboratories, Bothell, USA) using a broad-bandwidth (14-5 MHz) and a linear scanhead. Entire breasts were scanned by one of three radiologists, their experiences of breast imaging ranged from 3 to 10 yr. When a lesion was detected, it was saved in two different projections (transverse and longitudinal projections). A breast radiologist, 7 yr experience in breast imaging, reviewed the soft copies of US. Lesion sizes and characteristics were evaluated on a PACS system (StarPACS; Infinitt, Seoul, Korea). Lesion sizes were expressed as mean size±standard deviations. Tumor characteristics were assessed using the BI-RADS®-US lexicon (23): shape (oval, round, or irregular), margin (circumscribed, indistinct, microlobulated, angular, or spiculated), echo pattern (hypoechoic, isoechoic, or hyperechoic), posterior acoustic features (no posterior acoustic features, enhancement, shadowing, or combined pattern), orientation (parallel or not parallel to the skin), lesion boundary (abrupt interface or echogenic halo), and presence of microcalcifications.
One phyisician reviewed the clinical and pathologic reports of all 191 patients. Tumor staging was performed according to the TNM classification of breast cancer.(24) Primary tumor (T stage), regional nodal status (N stage), and metastasis (M stage) were evaluated. Data were collected on paper and then entered into a customized database (Microsoft® Access 2.0; Microsoft, Redmond, USA).
3. Statistical analysis
To compare the clinical and US findings of palpable and nonpalpable breast cancers, the chi-squared homogeneity test and the student's t-test were used, as appropriate. Statistical significance was considered if a p value was less than 0.05. A crude odds ratio (OR) and its 95% confidence interval (CI) were calculated for the presence of a palpable cancer based on each US finding. All statistical analysis was performed using SAS version 9.12 (SAS Inc., Cary, USA). The statistical analysis of the data was supervised by a biostatistician.
RESULTS
Table 1 presents patient characteristics. Patients' ages
were not different between the two groups (p=0.39). T and N stages were significantly poorer for palpable than nonpalpable breast cancers (p<0.05). Frequency of DCIS (Tis) was much higher for nonpalpable cancers (22/70, 31% vs 11/121, 9%), and lymph node negativity (N0) was more frequent in nonpalpable cancers (53/70, 76% vs 64/121, 53%). Overall breast cancer stage was also significantly poorer for palpable breast cancers (p<0.05). Moreover, the frequency of early cancer, stage 0 or 1, was significantly higher for nonpalpable cancers (p<0.05).
By breast US, the mean lesion size of palpable cancers was 27.03±20.56 mm and of nonpalpable cancers was 12.64±5.19 mm, and this difference was statistically significant (p<0.0001). By pathologic examination, mean tumor size of palpable cancers was 32.41±73.43 mm and of nonpalpable cancers 17.89±13.48 mm and this was significantly different (p<0.05).
Table 2 summarizes the US findings of palpable and
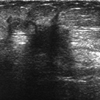
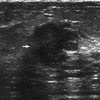
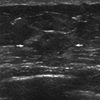
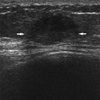
nonpalpable breast cancers. In terms of lesion characteristics by US, shape, margin, posterior acoustic features, and orientation were significantly different between the two study groups (p<0.05). An "irregular" shape was more frequent for palpable cancers (98/126, 78% vs 40/74, 54%; OR=2.98, 95% CI=1.60-5.54) (Fig 1, 2), whereas an "oval" shape was more common for nonpalpable cancers (24/74, 32% vs 18/126, 14%; OR=0.35, 95% CI=0.17-0.70) (Fig 3, 4). In lesion margins, a "spiculated" margin was significantly more commonly observed in palpable cancers (37/126, 29% vs 10/74, 14%; OR=2.66, 95% CI=1.23-5.74) (Fig 1). With respect to posterior acoustic features, a "combined pattern" was more frequent for palpable cancers (21/126, 17% vs 2/74, 3%; OR=7.20, 95% CI=1.64-31.66) (Fig 1, 2), whereas "no posterior acoustic features" was more common for nonpalpable cancers (44/74, 59% vs 53/126, 42%; OR=0.50, 95% CI=0.28-0.89) (Fig 3). A "not-parallel" orientation to skin was more common for palpable cancers (81/126, 64% vs 35/74, 47%; OR=2.01, 95% CI=1.12-3.60) (Fig 1, 2) and a "parallel" orientation was more common in nonpalpable cancers (39/74, 53% vs 45/126, 36%; OR=0.50, 95% CI=0.28-0.89) (Fig 3, 4). An "echogenic halo" (Fig 1, 2) and the "presence of microcalcifications" were more frequent in palpable than in nonpalpable cancers, but this was without significance (p>0.05).
DISCUSSION
The most important roles of US in breast imaging are; the characterization of masses that have been incompletely assessed by mammography, the characterization of palpable masses that are obscured by dense tissue during mammography, and screening for occult breast cancers in dense breasts by mammography. Breast US has been successfully used to differentiate benign and malignant breast lesions and to detect occult breast cancers in dense breasts.(15-22) Our question was that breast US would correlate with clinical findings and prognosis. There are a few reports to show correlation between tumor type or grade and US findings in breast cancers. (25, 26) Moon et al.(26) reported that DCIS cases have less often typical malignant US findings, thus, radiologists or sonographer may misunderstand the lesion as benign. In this study, we investigated the correlation of clinical palpability with breast US findings. It has been widely reported that palpable and nonpalpable breast cancers have different clinicopathological findings and prognoses.(1-5, 7) Skinner et al.(6) demonstrated that palpability is correlated with pathologic tumor size, mitotic grade, nuclear grade, lymphovascular invasion, nodal positivity, and the lack of an extensive intraductal component, multifocality, and multicentricity. They suggested that palpable cancers inherently differ from non-palpable cancers, and that they have a less diffuse growth pattern, higher metastatic potential, higher proliferative activity, more nuclear abnormalities, and a poorer prognosis. Moreover, the prognosis of nonpalpable cancers is better and their recurrence rate lower than those of palpable cancer.(2-5) Our results also demonstrate palpable breast cancers have a larger primary tumor size, a higher tumor stage, and are more frequently associated with lymph node metastasis.
In the present study, we evaluated differences between palpable and nonpalpable cancers in terms of their US characteristics; shape, margin, echo pattern, posterior acoustic features, orientation, lesion boundary, and presence of microcalcifications. Among these US characteristics, shape, margin, posterior acoustic feature, and orientation differed between the two study groups. An "irregular" shape (OR=2.98), "spiculated" margin (OR=2.66), "combined pattern" of posterior acoustic feature (OR=7.20) and "not-parallel" orientation (OR=2.01) were more frequent for palpable breast cancers; moreover, these are typical breast cancer US findings (22). Pathologic examinations show that palpable cancers are larger and have a higher stage than nonpalpable cancers, and that various internal components, such as, necrosis or hemorrhage, are more likely in palpable cancers. These typical US findings are caused by an enlarging tumor, tumor invasion to surrounding tissue, and various internal components. An "irregular" shape, a "spiculated" margin, and a "not-parallel" orientation are related with a stellate configuration, which is associated with desmo plastic reaction indicating tumor-associated fibrosis. Patients with abundant desmoplastic reaction show more frequent lymphovascular invasion, lymph node metastasis, and angiogenesis than those with a poor desmoplastic reaction, and thus a poorer prognosis.(27) A "combined pattern" of posterior acoustic feature means a combination of shadowing and enhancement. Shadowing is the result of sound beam attenuation by desmoplastic host response to breast cancer.(22) Enhancement is caused by highly cellular tumors and necrotic cancers.(22) Thus, a "combined pattern" of posterior acoustic feature in palpable cancers might be related with the presence of various cellular components, desmoplastic reaction, necrosis, and hemorrhage caused by angiogenesis. Thus, the different breast US characteristics of palpable and nonpalpable breast cancers might be related with pathologic differences and in turn be related with prognosis.
There are many reports to describe the usefulness of US in nonpalpable breast lesions for detection of malignancy and imaging-guided procedure.(15, 17-21, 28) However, there is no report to show that distinctive US findings for nonpalpable breast cancers when compared with palpable breast cancers. Our results demonstrated nonpalpable breast cancers had more often typical benign US findings; an "oval" shape, a "circumscribed" margin, "no posterior acoustic features", a "parallel" orientation, and an "abrupt" interface. Among these findings, an "oval" shape, "no posterior acoustic features", and a "parallel" orientation were significantly different between palpable and nonpalpable breast cancers. Therefore, physicians must consider these results before assessment of nonpalpable breast lesions on US and it may be necessary of more strict application of US criteria to nonpalpable breast lesions. If a nonpalpable lesion has a slight malignant feature on US, biopsy or aspiration should be considered.
The present study has several limitations. First, the study is limited by its retrospective nature. We included patients who underwent breast cancer surgery and breast US, and the total number of patients was small. Thus, a further prospective study in a larger population may be warranted. Second, the characteristics of palpable and nonpalpable cancers were compared by breast US, but these different US characteristics were not correlated with pathologic findings. Third, we included both invasive carcinomas and DCIS cases, thus, the study population was heterogeneous and it could produce biased results. In the 200 breast cancers, 167 were invasive carcinomas and 33 were DCIS cases. We hope further study would be performed in separate groups of histological tumor types.


 XML Download
XML Download