

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Enterococcus is a Gram-positive and common commensal bacterium of human gastrointestinal and genitourinary tracts [1]. Over the past two decades, enterococci have emerged as an important agent responsible for hospital acquired infection, particularly bacteremia, sepsis, endocarditis, urinary tract infection (UTI), and abdominal and pelvic infections [2]. Certain conditions, such as prolonged hospitalization, immunodeficiency and antibiotic therapy, causes a high risk for acquiring of enterococcal infections in patients [34].
Several virulence factors including enterococcal surface protein (Esp), hyaluronidase (Hyl), gelatinase (GelE), aggregation substance (AS) proteins (Asa1), collagen-binding protein (Ace), and cytolysin (CylA) contribute to the adherence, colonization, evasion of the host immune response, extracellular production of enzymes, pathogenicity, and severity of the infection [56]. Moreover, treatment of enterococcal infections has been clinically challenging due to increasing resistance to a broad range of antimicrobial agents, including β‑lactams, macrolides, fluroquinolones, glycopeptides, and aminoglycosides [47].
Enterococci possess efficient genetic exchange systems. The genes encoding virulence determinants can be transferred to resistant strains via these systems [48]. Emergence of antimicrobial resistant virulent enterococci is a serious problem in the treatment and control of nosocomial infections [9].
Several studies have shown that Enterococcus faecalis is an important and virulent species causing various infections [461011]. There are few data regarding the enterococcal virulence determinants in hospitalized patients in south-west of Iran. Therefore, the aim of the present study was to examine the prevalence of genes encoding virulence factors and antimicrobial resistance patterns of E. faecalis strains isolated from hospitalized patients in Shiraz, Iran.
Materials and Methods
1. Bacterial isolates
A total of 51 E. faecalis isolates were collected from specimens of patients hospitalized in Nemazee hospital (the main hospital affiliated to Shiraz University of Medical Sciences with 1,000 beds and 50,000 inpatients per year) during September 2015 to March 2016. They were obtained from the urine (n = 38), blood (n = 4), pleural fluid (n = 4), peritoneal fluid (n = 2), eye discharge (n = 1), endotracheal tube (ETT) (n = 1), and transjugular intrahepatic portosystemic shunt (TIPS) (n = 1). Only one isolate per patient was included. Identification of enterococcal isolates was performed based on conventional microbiological tests (Gram staining, catalase test, growth on Brain Heart Infusion agar (Conda, Madrid, Spain) with 6.5% NaCl, and bile-esculin test) [1213]. The ddlE gene was targeted by polymerase chain reaction (PCR) using species specific primers (ddlE. faecalis F-5'-ATCAAGTACAGTTAGTCT-3' and R-5'-ACGATTCAAAGCTAACTG-3') for molecular confirmation of E. faecalis [414]. The PCR protocol consisted of a pre-denaturation step at 95 °C for 5 min, followed by 30 cycles of 60s at 95°C, 45s at 45°C and 50s at 72°C. A final extension step was performed at 72°C for 5 min.
2. Antimicrobial susceptibility testing
Antimicrobial sensitivity tests were performed by disc diffusion method on the Mueller- Hinton Agar (Merck Co., Darmstadt, Germany) based on Clinical and Laboratory Standards Institute (CLSI) guideline [15]. The tested antibiotics (Mast Group Ltd., UK.) were penicillin (10 units), ampicillin (10 µg), ciprofloxacin (5 µg), erythromycin (15 µg), tetracycline (30 µg), nitrofurantoin (300 µg), rifampin (5 µg), fosfomycin (200 µg), quinupristin- dalfopristin (15 µg), linezolid (5 µg), vancomycin, (30 µg) and teicoplanin (30 µg). High-level gentamicin resistant (HLGR) isolates were also detected by disc diffusion method (with 120 µg gentamicin disks) on the Mueller- Hinton Agar (Merck Co., Darmstadt, Germany) [15]. E. faecalis ATCC 29212 was used as the reference strain for antibiotic susceptibility testing.
3. DNA extraction and detection of virulence genes
Genomic DNA was extracted from fresh colonies as described previously [4]. PCR was done for detection of the genes encoding virulence factors (esp, cylA, hyl, gelE, asa1, ace, efa) [48]. The products were separated by electrophoresis in 1.5% agarose gels with 1 X TAE (Tris/Acetate/EDTA) buffer, stained with KBC power load dye (CinnaGen Co. Tehran, Iran) and visualized under ultraviolet illumination.
4. Statistical analysis
The distribution of virulence genes among HLGR and non-HLGR isolates was calculated by Chi-square and Fisher's exact test for each gene. In addition, differences in the incidence of virulence genes with respect to the origin of specimen were also analyzed by Chi-square test. A P-value of ≤0.05 was considered as statistically significant.
Results
1. Antimicrobial resistance pattern
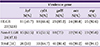
During 6 months of the study, a total of 51 E. faecalis strains were collected randomly with the possibility of true infections. No isolate was found to be resistant to fosfomycin and linezolid. Vancomycin resistance was observed among 23 (45.1%) isolates (Table 1). More than half of the isolates (52.9%) were HLGR (Table 2).
Table 1
Antimicrobial resistance rates among Enterococcus faecalis isolates.
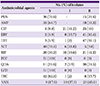
Table 2
The distribution of virulence genes and high level resistance to gentamicin among Enterococcus faecalis isolates.

2. Distribution of virulence genes
The efa and asa1 were the most frequently detected gene (100%) among isolates, followed by esp (94.1%), ace (90.2%), gelE (80.4%), cylA (64.7%), and hyl (51%) (Table 2). The frequency of genes encoding virulence factors among HLGR and non-HLGR isolates is shown in Table 3. There was no significant difference between the distribution of virulence genes among HLGR and non-HLGR isolates (P > 0.05).
Table 3
Distribution of genes encoding virulence factors among HLGR and non-HLGR isolates.
Discussion
Enterococci, particularly E. faecalis, are common pathogens that can cause severe nosocomial infections [7]. In our study, E. faecalis isolates were obtained from various clinical specimens. Similar to other reports from Iran, noticeable resistance to several antimicrobial agents among E. faecalis strains was observed [416]. Nearly half of the isolates were resistant to vancomycin (45.1%). Similarly, high prevalence of vancomycin-resistant enterococci has been previously reported from southwestern Iran [1317]. All of isolates were susceptible to fosfomycin and linezolid (Table 1). Our findings indicate that these agents are efficient choices against enterococcal infections.
More than 52% of the strains were HLGR. Resistance to high concentrations of gentamicin among E. faecalis isolates has been reported in previous studies [89] Presence of genes encoding aminoglycoside-modifying enzymes and transmission among enterococcal strains lead to high levels resistance to gentamicin [18]. It seems that gentamicin has become an ineffective antibiotic against hospital-acquired enterococcal infections.
In addition to antimicrobial resistance, the presence of virulence factors is another concern about enterococci that may contribute to the severity of enterococcal infections [8]. In the present study, the distribution of virulence genes among E. faecalis strains was determined.
All of the isolates harbored efa and asa1 genes (Table 2). In various studies, similar frequencies of the efa have been reported [489]. In a study conducted by Gaglio et al., the efa gene was detected among 25% of the strains isolated from dairy products [19]. It appears that the efa gene is always present in clinical E. faecalis strains. In the current study, the prevalence of asa1 was more than that observed in previous studies [48192021]. AS encoded by asa1 causes clumping of E. faecalis strains and mediates efficient DNA exchange between donor and recipient bacteria [522]. The presence of asa1 gene among all of our isolates can facilitate exchange of resistance and virulence associated genes in hospital setting.
The esp was the second most detected gene among the isolates (94.1%). The prevalence of esp was also 94.7% in strains isolated from UTI. High frequency of esp among UTI causative E. faecalis isolates is consistent with other studies [623]. The enterococcal surface protein is encoded by the esp gene facilities colonization and persistence of E. faecalis in acute urinary tract infections [524].
We found that the prevalence of ace, gelE, cylA and hyl genes was 90.2%, 80.4%, 64.7%, and 51%. Our results indicated that E. faecalis isolates carried more virulence genes in comparison to various reports [49181925262728]. These differences probably reflect variability in the types of samples or geographic regions.
There was no significant difference between the distribution of virulence factors among HLGR and non-HLGR isolates, although cylA and gelE were more prevalent in HLGR strains (Table 3). This result is in contrast with that of a previous study which has reported that the hyl gene is significantly the most frequent virulence gene in HLGR isolates [4].
In the current study, the antimicrobial resistant isolate obtained from TIPS had 6 virulence genes. Colonization of same isolates in hospital environment may lead to life threatening infection in hospitalized patients. Therefore, to prevent colonization of such drug resistant virulent isolates, infection control procedures should be performed.
To the best of our knowledge, this study is the first investigation regarding enterococcal virulence determinants in Shiraz, the south west of Iran. Moreover, high virulence strains were identified. Different profiles of virulence factors can be important for understanding the enterococcal pathogenicity and their effects on the host.
There were some limitations related to the present study. First, small number of isolates were investigated. Second, to identification of the source of infection and take preventive measures in hospital setting molecular analysis was required.
In conclusion, a high incidence of genes encoding virulence factors among E. faecalis strains isolated from clinical samples was observed. Our results indicated that all of the isolates carried efa and asa1 genes. The esp was the second most prevalent one. Gene encoding Hyl (hyl) was the least frequent one that presented in more than half of the isolates. To prevent colonization of such virulent strains in hospital environment, infection control procedures are recommended to be performed.
 XML Download
XML Download