

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Acute pyelonephritis (APN) refers to infection of the renal pelvis and the parenchyma. It generally occurs due to ascending infection via the bladder [12]. The annual prevalence of acute pyelonephritis in Korea is 35.7/10,000 people, and is higher in women than in men (59/10,000 vs. 12.6/10,000) [3]. The disease is diagnosed by identifying the pathogen in urine cultures, as well as by the clinical symptoms of fever, flank pain, costovertebral angle (CVA) tenderness and urinary symptoms such as frequency of urination, urgency, and dysuria [4]. In addition, blood cultures are commonly conducted in patients with APN, but the usefulness of these has not been supported in several reports [2567]. However, the utility of the test may differ according to the host, antibiotic exposure before hospital visit and rate of positive culture.
Radiologic imaging studies such as computed tomography (CT) and renal ultrasonography (US) are conducted to diagnose structural problems such as ureteral obstruction or renal abscess in some patients with unsatisfactory clinical response to antibiotic treatment [2].
The aforementioned diagnostic tools have been widely used in clinical practice, but little is known about how frequently they are used and whether they influence the management of APN patients. Accordingly, this prospective study was conducted in a cohort of community-acquired APN (CA-APN) patients to examine the usefulness of blood cultures and radiologic imaging studies for making therapeutic decisions.
Materials and Methods
Clinical data on CA-APN patients were collected from 11 general hospitals with 500-1,250 beds from March 2010 to February 2011. Ten of the 11 hospitals were university hospitals. The study protocol was reviewed and approved by the Institutional Review Boards (IRBs) of the participating hospitals. Personal information was encrypted, and informed consent was waived by the IRBs.
Patients with fever ≥37.8˚C who satisfied at least 3 of the following 5 conditions were included in this study: (1) frequency of urination, dysuria, or suprapubic tenderness as symptoms of lower urinary tract infection; (2) flank pain; (3) CVA tenderness; (4) pyuria defined as white blood cell (WBC) count ≥10 in a high power field in urinalysis; and (5) leukocytosis defined as WBC count ≥20,000/mm3 or polymorphonuclear cell count ≥ 65% in peripheral blood tests [89]. Patients under 15 years old, those with other reasons for pyuria and fever, and those with insufficient data were excluded. The study subjects were clinically diagnosed by infectious disease experts in the participating hospitals.
Urine and blood cultures were processed at the time of admission. Etiologic agents were determined when organisms at ≥105 colony forming unit (CFU)/mL were identified in urine cultures and/or urinary pathogens were isolated from blood cultures. Species identification and susceptibilities to antimicrobial agents were determined by means of a semiautomated system (VITEK, bioMerieux, Hazelwood, MO, USA; or Microscan, DADE Behring, West Sacramento, CA, USA) [10]. CT was considered diagnostic for APN if single or multiple hypodense parenchymal areas were seen after infusion of contrast medium , and local low-echo contrast with an unclear boundary caused by renal interstitial edema was diagnostic in abdominal US [11] performed by radiologists in each hospital.
The patients' demographics, disease history, clinical symptoms and signs, and treatment outcomes were prospectively collected via a web-based medical records system. Disease history included antibiotic use, history of urinary treat infection (UTI), and history of admission in the past year. The clinical symptoms and signs included flank pain, signs of lower urinary tract infection, CVA tenderness, and nausea/vomiting. Pitt score was made up of: (1) oral temperature (2 points for ≤35°C or ≥40°C, 1 point for 35.1-36.0°C or 39.0-39.9°C, and 0 point for 36.1-38.9°C); (2) acute hypotension (2 points for an systemic blood pressure decrease >30 mmHg and a diastolic blood pressure decrease >20 mmHg; (3) ventilator use (2 points); (4) heart failure (4 points); and (5) consciousness (0 point for alertness, 1 point for disorientation, 2 points for stupor, and 4 points for coma) [12]. Azotemia was defined as serum blood urea nitrogen (BUN) ≥20 mg/dL and/or serum creatinine ≥2.0 mg/dL. Discordant therapy was defined as cases whose empirical antimicrobial therapy regimen was changed due to the drug resistance. Variables reflecting clinical outcome included final clinical failure, hospital mortality, hospitalization days, and time to fever clearance. Final clinical failure was defined as recurrence of symptoms of UTIs within 7-14 days of follow-up, or death.
In terms of evaluation of the diagnostic tests, positive rates and agreement between urine and blood culture were investigated, and positive rates of abdominal US and CT were examined. In addition, we assessed whether the above diagnostic tests affected therapeutic decisions such as interventional treatment or treatment duration. In connection with the radiologic findings, structural abnormalities were defined as lesions which could potentially impact treatment duration or modalities such as urolithiasis, hydronephrosis/hydroureter, renal abscess, perinephric abscess and emphysematous nephritis or cystitis.
Statistical methods: Categorical variables were compared with the Chi-square test or Fisher's exact test, and continuous variables with the Mann-Whitney tests. Univariate and multivariate logistic regression analysis was performed using backward method. A P-value of <0.05 was considered statistically significant. Statistical analyses were conducted using SPSS version 18.0 for Windows (SPSS Inc., Chicago, IL, USA).
Results
A total of 827 patients with CA-APN were enrolled. Their demographic characteristics, underlying diseases and past histories are summarized in Table 1.
Table 1
Demographics and underlying diseases of the study subjects

1. Performance and positive rates of urine and blood cultures
Urine and blood cultures were carried out in 820 (99.2%) and 648 (78.4%) of the 827 patients, respectively, and the positive rates were 69.3% (568/820) and 42.7% (277/648), respectively (Table 2). Escherichia coli was the most commonly isolated pathogen in both urine and blood cultures: 90.1% (512/568) in urine and 82.7% (229/277) in blood. Among 225 patients with positive urine and blood cultures, the organisms isolated from urine were consistent with those isolated from blood in 214 patients (95.1%), but inconsistent in 11 patients (4.9%). Of the 645 patients who underwent both of urine and blood cultures, 49 (7.6%) were diagnosed via their blood cultures because their urine cultures were negative. The initial antibiotic regimen was modified in 179 patients (21.7%), 95 of whom changed regimen because of the results of antimicrobial susceptibility tests: 15 patients (15.8%) after blood culture results and 80 (84.2%) after urine culture results.
Table 2
Positivity of cultures of blood and urine

2. Clinical influence of positive blood cultures on the patients with CA-APN
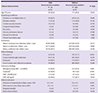
We investigated the effect of bacteremia on disease course among the 648 patients from whom blood cultures were obtained, by dividing them into those with bacteremia and those without bacteremia according to the culture results. Clinical characteristics and treatment outcomes of the two groups were compared (Table 3). The numbers of elderly patients ≥ 70 years and those with a Charlson comorbidity index ≥1 were higher in the bacteremia group than the non-bacteremia group, and clinical illness was more severe in the former: there were more patients with Pitt score ≥1, WBC count ≥20,000/mm3 and C-reactive protein (CRP) ≥20 mg/dL in the bacteremia group. Accordingly, final clinical failure was more common in the bacteremia group (8.0% vs. 2.7%, P = 0.003) and deaths were also more frequent: 3.6% (9/251) vs 0.3% (1/338). Likewise, durations of hospitalization and fever were also longer in the former group. For evaluation of clinical effect of bacteremia on clinical outcomes including hospital mortality and final clinical failure, univariate and multivariate logistic regression test was performed (Table 4). Input variables was included as follows: age ≥70 years, Chalson comorbidity index ≥1, diabetes mellitus, chronic renal disease, WBC ≥20,000/mm3, CRP ≥20 mg/dL, positive blood culture and discordant therapy. Among above variables, positive blood culture was significant predictor for hospital mortality (OR 9.290, 95% CI 1.145-75.392, P = 0.037), although not for final clinical failure.
Table 3
Comparison of the clinical features of the CA-APN patients with positive and negative blood cultures
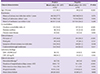
Table 4
Risk factors related to mortality in Community-acquired acute pyelonephritis

3. Results of radiologic imaging studies
Of the 872 patients with CA-APN, 683 (78.3%) underwent abdominal CT (503, 57.7%), abdominal US (154, 17.7%) or both (24, 2.8%) within 7 days of admission. Abdominal CT was conducted in 527 patients at median 0 day (range, 0-7 days) after they visited the hospital because of: an uncertain diagnosis in 339 patients (64.3%), suspected structural abnormality in 86 (16.3%), persistent fever after 72 hours of antibiotic use in 20 (3.8%), male gender and adolescence in 32 and 4 (6.1%, 0.76%), respectively, severe sepsis in 19 (3.6%) and other reasons in 27 (5.1%). Abdominal US was conducted in 180 patients at median 1 day (range, 0-8 days) after hospital visit, due to diagnostic uncertainty in 74 patients (41.1%) and suspected structural abnormality in 30 patients (16.7%). Final radiologic findings were in Table 5. The APN detection rates were 84.4% (445/527) and 40% (72/180) by abdominal CT and abdominal US, respectively. As the final outcome of the radiologic imaging studies, 21 (4.0%) of the 527 patients undergoing abdominal CT and 5 of the 180 patients undergoing abdominal US (2.8%), respectively, underwent interventional procedures.
Table 5
Radiologic findings in abdominal computed tomography and abdominal ultrasonography

4. Clinical characteristics of the CA-APN patients with structural abnormalities
In order to identify patients whose treatment might need to be modified by, for example, extending the treatment or carrying out interventional procedures, we compared the clinical characteristics of 81 patients with structural abnormalities, such as renal abscess, perinephric abscess, urolithiasis, hydronephorosis/hydroureter and emphysematous cystitis, with those of 602 patients without such lesions (Table 6). Patients with Pitt score ≥1, flank pain and azotemia were significantly more likely to have structural abnormalities that could potentially impact on treatment modalities. With regard to clinical outcomes in the 2 groups, defervescence time (3.5 vs. 2.5 days, P = 0.001) and duration of hospitalization (11.5 vs. 8.8 days, P <0.001) were significantly longer in the group with structural abnormalities, but there was no difference in final clinical failure or hospital mortality. For the evaluation of relationship between the early clinical failure and structural abnormalities, sub-group analysis was performed with 30 patients who underwent imaging studies for the reason of non-response of therapy after 72 hours. We divided into two groups depending on the structural abnormalities, and compared their clinical characteristics. However, there were no significant differences including final clinical failure and hospital mortality between two groups (data not shown).
Table 6
Clinical characteristics of the CA-APN patients with structural abnormalities
aSee method for calculation of Pitt score
bAzotemia was defined as serum BUN ≥ 20 mg/dL and/or serum creatinine ≥ 2.0 mg/dL.
CA-APN, community-acquired acute pyelonephritis; RBC, red blood cell; HPF, high-power field; WBC, white blood cell; CRP, C-reactive protein; SD, standard deviation; BUN, blood urea nitrogen.
Discussion
APN is diagnosed by clinical signs and symptoms of upper urinary tract infection, and isolation of the pathogen from urine [4]. In clinical practice, blood cultures and radiologic imaging studies such as CT are commonly used [5613]. Although these tests have been performed on a substantial number of patients, there has been controversy as to their accuracy and usefulness. The purpose of this study was to evaluate the impact of blood cultures and radiologic tests on the management of CA-APN patients.
Retrospective studies have found that, generally, 70-90% of CA-APN patients undergo blood cultures [714]. Several reports have evaluated the usefulness of blood cultures in women with uncomplicated APN, and proposed that blood cultures do not provide additional useful information for clinical managements [2571415], as was also reported in the case of pregnant women with APN [16]. Even in complicated APN patients with structural or functional urinary tract abnormalities, blood cultures have limited value for treatment choices [6]. One report has shown that complicated CA-APN patients with bacteremia had more severe clinical manifestations with more severe sepsis or septic shock, resulting in longer defervescence and hospitalization times than those without bacteremia [17]. In the present study, different microorganisms were isolated from urine and blood cultures in 11 patients, and in 49 patients pathogens were isolated from blood only; therefore, blood cultures provided important information in 60 of the 645 patients (9.3%) in whom both urine and blood cultures were performed. Since quite a few patients coming to a tertiary hospital via a primary clinic have already been prescribed antibiotics, the 49 patients yielding only positive blood cultures could be explained by the fact that they had already taken sufficient antibiotic to sterilize their urine but not to their blood. Indeed, the positive rate of urine culture was lower (69.3%) in this report than in the aforementioned reports. Furthermore, CA-APN patients with positive blood culture were shown worse clinical outcomes and bacteremia was independent risk factor for hospital mortality in this study.
With regard to radiologic imaging studies for CA-APN, the American College of Radiology recommends waiting for 72 hours before carrying out any imaging [1819], and proposes CT as the imaging method of choice for diagnosing patients with atypical pyelonephritis [18]. Abdominal CT increases the sensitivity and specificity of diagnosis of APN, which enables confirmation of early lesions and is useful for locating the anatomical lesions in infected tissues and confirming abscesses and perirenal inflammation. Abdominal US has low sensitivity for detecting early APN but avoids radiation exposure, may be used in pregnant mothers and in children, and is useful for detecting renal parenchymal inflammation and confirming abscess formation [1120]. Generally, radiologic tests are performed in the following cases: 1) patients that are unresponsive in the first 72-hours of treatment, 2) intervention-requiring patients with structural and functional abnormalities of the urinary system, 3) high-risk patients with diabetes mellitus, old age, or taking immunosuppressants, and 4) cases requiring confirmation of bacterial infection infiltrating other organs [21]. However, intervention-requiring pyelonephritis patients could not be identified prior to imaging study. In a report that found very low rates of positive urine or blood cultures, CT and nuclear magnetic resonance were proposed as tools for diagnosis of APN, especially for detecting progression to abscess [13].
In this study, US and CT scans were carried out in more than 80% of CA-APN patients regardless of their responses to treatment, and mostly within 3 days. When we compared the demographic and clinical characteristics of the groups that did and did not undergo radiologic testing, we found no difference (data not shown), which suggests that clinicians did not follow any consistent principle in ordering radiologic tests. The rate of detection of infections in the kidney by US was very low, and CT missed over 10% of APN in this study, probably because most radiologic studies were performed early in the disease course. Nevertheless, radiologic imaging detected 81 patients (11.9%) with structural abnormalities which could potentially impact on clinical management, such as interventions and extension of treatment, among 683 patients with CA-APN. The prevalence of structural or functional abnormalities in CA-APN may vary according to the patient population, and the characteristics of the medical center or community; the 11.9% prevalence in this study was probably due to the fact that most of the enrolled patients were hospitalized and all but one of the institutions involved were university-affiliated tertiary hospitals. Nevertheless, we were able to identify clinical features that were more common in patients with structural abnormalities, namely Pitt score ≥1 and presence of flank pain or azotemia. Therefore, it might be helpful to use these abnormalities as indicators for deciding whether to carry out early radiologic studies in clinical practice.
The significance of this study is that it is a prospectively performed multi-center study of a large number of cases of CA-APN aiming to assess the impacts of blood cultures and radiologic imaging studies on therapeutic decision-making. Although it was principally an observational study without intervention, more than 80% of the patients underwent radiologic imaging studies. Because of this overuse of these tools, we were able to analyze the radiologic findings in a large number of CA-APN patients. However, this study also has a potential limitation in that most of the patients were hospitalized in a tertiary university hospital, and the patient population might have had on average a severe form of CA-APN. In addition, the impact of posivive blood culture tests on severe sepsis or septic shock was not assessed due to lack of collecting variables.
In conclusion, blood cultures performed early were clinically useful for diagnosing CA-APN, and bacteremia is predictive factor for hospital mortality. In terms of radiologic studies, more than 10% of the patients had structural abnormalities potentially influencing clinical management. Early radiologic imaging studies should be considered for CA-APN patients with Pitt score ≥1, or have flank pain or azotemia.
 XML Download
XML Download