

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Enterococci are considered normal flora in human and animal intestine. Although Enterococcus faecalis has been reported in 65-80% of enterococcal infections [1], one report showed that E. faecalis causes nearly half (not the most) of all enterococcal infections [2]. The contribution of some species might be different in some countries. The pathogenesis of enterococci has been attributed to different factors such as antibiotic resistance, biofilm formation and the presence of some adhesive and secreted agents.
Extracellular surface protein (ESP) is one of the most important adhesions involved in colonization and biofilm formation [3]. Cytolysin (CylA) and gelatinase (GelE) are secreted factors implicated in the pathogenesis of Enterococcus species. It has been suggested that gelatinase and the other peptides might play an important role in the severity of systemic enterococcal diseases [34]. In addition, E. faecalis strains that produce hemolysin and show cytolytic activity have been shown to be more virulent in humans and more associated with infections of increased severity [5].
Biofilms and as the other virulence factors could promote infections and increase tolerance to antimicrobial agents and host immune responses [6]. The role of different enterococcal factors in biofilm formation has been investigated. However, no definite conclusions have been published [37]. The aim of this study was to evaluate the ability of biofilm formation in E. faecalis isolates collected from pathogenic and fecal samples. In addition, the profile of their virulence genes was determined, and the relation between virulence profile and biofilm formation was evaluated.
Materials and Methods
One hundred and twenty-three Enterococcus spp. were collected from different patient specimens, including urine, blood, wound, body fluids and trachea. Enterococci were isolated in pure cultures and found to be the cause of true infection in all the cases. Additionally, 89 Enterococcus spp. were isolated from fecal samples of healthy people (known as colonizer isolates). All isolates were initially identified by conventional biochemical tests, including Gram staining, catalase reaction, growth in the presence of 6.5% NaCl, bile esculin hydrolysis and fermentation of arabinose [8]. The ddlE.feacalis
gene was amplified by PCR to confirm the identity of the isolates [9] (Table 1).
Table 1
Primers and amplification conditions for PCR assay

| Target gene |
Primer pair sequences 5'→3' |
PCR product (bp) | PCR condition | Reference |
|---|---|---|---|---|
| ddlE.faecalis | ATCAAGTACAGTTAGTCT | 941 | 94℃ 60 s, 54℃ 60 s | [9] |
| ACGATTCAAAGCTAACTG | 72℃ 60 s, 30 cycles | |||
| vanA | CATGAATAGAATAAAAGTTGCAATA | 1,030 | 94℃ 60 s, 54℃ 60 s | [15] |
| CCCCTTTAACGCTAATACGATCAA | 72℃ for 60 s, 30 cycle | |||
| vanB | GTGACAAACCGGAGGCGAGGA | 433 | ||
| CCGCCATCCTCCTGCAAAAAA | ||||
| esp | AGATTTCATCTTTGATTCTTGG | 510 | 94℃ 60 s, 56℃ 60 s | [16] |
| AATTGATTCTTTAGCATCTGG | 72℃ 60 s, 30 cycles | |||
| cyl | ACTCGGGGATTGATAGGC | 688 | ||
| GCTGCTAAAGCTGCGCTT | ||||
| gelE | TATGACAATGCTTTTTGGGAT | 213 | ||
| AGATGCACCCGAAATAATATA |
1. Antimicrobial susceptibility testing
The disk diffusion test was employed to determine the susceptibility of the isolates to vancomycin (30 µg), teicoplanin (30 µg), gentamicin (120 µg), linezolid (30 µg), ciprofloxacin (5 µg), erythromycin (15 µg), ampicillin (10 µg), tetracycline (30 µg) and rifampicin (5 µg) (Mast Group Ltd., Merseyside, UK). The microdilution broth method was used to determine the minimal inhibitory concentration (MIC) of vancomycin for the isolates that showed resistance phenotype after the disk diffusion method. The results were interpreted according to the guidelines of the Clinical and Laboratory Standards Institute (CLSI) [10]. Isolates that showed intermediate levels of susceptibility were classified as non-susceptible. Multidrug-resistance (MDR) was defined as resistance to three or more different classes of antibiotics [11].
2. Phenotypic assays
1) Gelatinase production
Gelatinase activity was determined, as described previously [12]. Briefly, the isolates were inoculated into a brain heart infusion broth (Merck, Darmstadt, Germany) containing 4% gelatin (40 g/L). After overnight incubation at 37ºC, the tubes were cooled at 4ºC for 30 min and gelatinase production was assessed by liquefying the gelatin.
2) Hemolysin production
The hemolytic activity was determined using blood agar plates after 24 or 48 h of incubation at 37ºC. The appearance of a clear zone of hydrolysis was considered indicative of β-hemolysis [13].
3) Biofilm formation
Semi-quantitative microtiter plate assay was performed, as described previously [14], with minor modifications. Briefly, the bacterial isolates grown on a trypticase soy agar (Merck, Germany) were diluted (1: 100) in a trypticase soy broth supplemented with 1% glucose. From this culture, 200 µl was inoculated into 96-well polystyrene flat-bottom microtiter plates (Guangzhou Jet Bio-Filtration Products Co., Ltd. Guangdong, China). After 24 h of incubation at 37ºC, the plates were gently washed thrice with sterile phosphate-buffered saline (PBS). The plates were inverted and left to dry for 1 h at 25ºC. For biofilm quantification, 200 µl of 2% aqueous safranin dye (Merck, Germany) solution was added to each well and the plates were allowed to stand for 40 min at room temperature. The excess safranin was washed off with sterile PBS, and the biofilm-bound-safranin was extracted with 200 ml of 95% ethanol. The absorbance of the extracted safranin was measured at 490 nm with an ELISA reader (BioTek, Vermont, USA). Optical density (OD) ≥ 0.24 was considered indicative of strong biofilm formation, and samples with OD ≤ 0.12 was categorized as non-biofilm-forming [14]. As a negative control, well-bound safranin was measured for wells exposed only to a medium containing TSB + 1% glucose, without any bacterial inoculation. Staphylococcus epidermidis RP62A was used as a positive control. All biofilm assays were carried out in triplicate.
3. Molecular assays
For all PCR experiments, genomic DNA was extracted using an appropriate DNA extraction kit (Cinnagen, Karaj, Iran), according to the manufacturer’s instruction. The absorption of the extracted DNA was measured at 260 nm and 280 nm, to confirm the quality of the product.
PCR amplification was conducted in a temperature-gradient thermal cycler (Biometra-T300, Gottingen, Germany), with a total volume of 50 µl. Each 50-µl PCR mixture consisted of 2 µl of bacterial DNA, 0.2 µM of each specific primer, and 25 µl of 2× Master Mix Red (Ampliqon, Odensem, Denmark); the master mix consisted of 0.2 unit/µl of AmpliqonTaq DNA polymerase, 1.5 mM MgCl2, and 0.4 µM dNTPs. After amplification, 5 µl of the PCR product was electrophoresed on a 1.5% agarose gel in 0.5× TBE buffer (5.4 g Tris base, 2.75 g boric acid, and 2 ml 0.5-M EDTA, in 1 L). The DNA ladder was a ready-to-use plasmid double digest of 100-3000 bp, which was obtained from SMOBIO Technology (Hsinchu, Taiwan). The specificity of the primers was verified using the Primer Quest software tool (http://www.ncbi.nlm.nih.gov/Gene).
1) Detection of vanA and vanB genes
A multiplex PCR assay was performed as described above, to detect two major vancomycin resistance determinants (vanA and vanB) in vancomycin-resistant E. faecalis (VRE) isolates, as described previously [15] (Table 1). E. faecium (CCUG 36804) and E. faecalis (CCUG 34062), kindly provided by Helen Edebro (Department of Clinical Microbiology, Umea University, Sweden) were used as positive strains for vanA and vanB, respectively.
4. Statistical analysis
The distribution of virulence genes in the clinical and commensal samples was calculated using the Chi-square and Fisher's exact tests for each gene. In addition, the differences in the incidence of virulence genes and biofilm formation, with respect to the type of specimen, were also analyzed using the Chi-square test. P ≤ 0.05 was considered statistically significant.
Results
Of the 123 Enterococcus spp. isolated from patient specimens, 84% (n = 103) were confirmed to be E. faecalis. Additionally, E. faecalis was identified in 22.5% (n = 20) of the fecal isolates. The majority of pathogenic E. faecalis isolates were found in urine (n = 74, 71.84%), followed by blood (n = 14, 13.59%), wound (n = 5, 4.85%), body fluids (n = 5, 4.85%), and trachea (n = 2, 1.94%). The origins of three isolates were unknown.
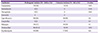
As shown in Table 2, among clinical isolates, the highest rates of non-susceptibility were found against ciprofloxacin (93%), erythromycin (89%), and tetracycline (83.5%). This pattern was slightly different in fecal isolates, where ciprofloxacin (90%), erythromycin (85%), and rifampicin (50%) were the most prevalent. All isolates were found to be susceptible to linezolid. In this study, 4 VRE isolates (MIC ≥256 µg/ml) were detected in urine (n = 2), blood (n = 1), and cerebrospinal fluid (n = 1). The presence of vanA was detected in all VRE isolates. All VRE isolates were also resistant to gentamicin, ciprofloxacin, tetracycline, erythromycin, and teicoplanin. High-level gentamicin resistance (HLGR) was found among 37% (n = 38) and 10% (n = 2) of pathogenic and fecal isolates, respectively. MDR was observed in 32% (n = 33) of the pathogenic isolates, which were most frequently from urine (76%, n = 25), of which 67% (n = 22) did not produce biofilm. In contrast, 5 (25%) fecal isolates showed MDR phenotype, among which three formed biofilm. However, a statistically significant correlation was not observed between biofilm formation and MDR phenotype (P = 0.146). The esp, gel, cyl genes were detected in 78.3%, 75.6%, and 45.9% of MDR isolates, respectively. No differences were observed between MDR and other isolates, in the presence of these genes (P ˃0.05).
Table 2
Antimicrobial non-susceptibility profiles of pathogenic and colonizer Enterococcus faecalis isolates
The distribution of virulence factors, gelatinase activity and biofilm formation is shown in Table 3. Overall, 71.5% (88/123) of the isolates carried gelE, of which 42% (37/88) displayed gelatinase activity. The esp gene was identified in 80.5% (99/123) of isolates, while 41% (50/123) carried the cyl gene. Furthermore, 45.5% (56/123) of the isolates formed biofilm. Most fecal isolates (90%, n = 18) were moderate or strong biofilm formers. In contrast, the most prevalent pathogenic isolates (63%, n = 65) did not produce any biofilm. Although no differences were observed between invasive and non-invasive isolates in biofilm formation, statistically significant differences were found between pathogenic and fecal isolates (P <0.001) (Table 3).
Table 3
Comparison between biofilm production, gelatinase activity and the presence of esp, cyl and gelE genes among invasive, non-invasive and colonizer Enterococcus faecalis isolates
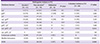
Additionally, biofilm formation was not associated with the presence of the esp (P = 0.587), gelE (P = 0.073) and cyl (P = 0.948) genes. Five pathogenic isolates that were strong biofilm producers and 2 fecal isolates that were weak biofilm formers did not contain any virulence genes, while 22 isolates from pathogen samples and one from a fecal sample harbored all the studied virulence genes, but did not form biofilm. Hemolytic activity was detected in 38% of cyl-positive isolates, with a tendency to be present more often in pathogenic isolates than in fecal isolates.
Discussion
E. faecalis is known to be the major cause of enterococcal infections, and has more prevalence than any other enterococcus species [117]. Antibiotic-resistant enterococci, particularly multi-drug resistant isolates, are now the leading cause of nosocomial infections worldwide [18]. The presence of multidrug resistant enterococci, particularly VRE and high-level gentamicin resistant isolates, is a serious problem, as they reduce the number of treatment options for enterococcal infections [19]. In this study, we found that many MDR isolates did not produce biofilms, which might indicate a relationship between virulence-associated genes and bacterial fitness. Although this relationship is unknown, it is likely to be complex and varies depending on the same factors. For example, a determinant that confers the ability to invade a host to Staphylococcus aureus may be associated with a fitness disadvantage, as invasion could lead to bacterial death following antibiotic treatment or host death. Expression accessory genes that are important for pathogenesis, but not critical for survival, may impose a cost to fitness through additional gene replication and protein secretion, if expressed during periods of carriage [20]. It is worth noting that antibiotic resistance alone cannot explain the virulence of enterococci; several other factors are also involved in this multifactorial process [21]. This study focused on detecting some of these factors, including the ability for biofilm formation, gelatinase and hemolysin production, and the presence of genes encoding the enterococcal surface protein (esp), gelatinase (gelE), and cytolysin (cyl) in pathogenic and fecal isolates. Additionally the correlation between biofilm formation and these virulence factors was investigated.
The prevalence of biofilm formation previously reported in pathogenic isolates is variable [72223]. In this study, the prevalence of biofilm production was 37% and 90% in pathogenic and fecal isolates, respectively. Although biofilm formation was not different between invasive and non-invasive isolates, there was a significant difference between pathogenic and fecal isolates (P <0.001). Johansson and Rasmussen [24] had shown that isolates from normal flora produced more biofilm than isolates from samples with infective endocarditis, which is consistent with our results. It can be assumed that virulence traits other than adherence are more relevant for pathogenic isolates. Studies on the role of esp in biofilm formation have had conflicting results. Some studies have demonstrated an association between biofilm formation and esp [12526], while others have shown that biofilm formation may occur independent of this protein [2728]. Our study was consistent with the latter group of studies, as no association was observed among the pathogenic and fecal samples (P ˃ 0.05). In addition, some studies have implicated other genes such as bopD, epa, and icaA in biofilm formation in E. faecalis [293031]. Similar to esp, the correlation between biofilm formation and gelE is controversial [21]. It has been shown that gelatinase activity, which is mediated by gelE [14], could affect the virulence and biofilm formation in enterococci [32].
In contrast, Ballering [33] had demonstrated that gelE was not linked to this phenotype. In our study, gelE was present in 72% of the pathogenic isolates (74/103), whereas gelatinase activity was detected in only 34% (35/103) of them. Interestingly, none of fecal isolates produced this enzyme; however, gelE was found in 55% (11/20) of them. Therefore, our results, along with those of Marra et al. [12], suggested that gelE was not necessarily responsible for gelatinase activity. This lack of gelatinase phenotypic/genotypic congruence has also been observed in some other studies [3435]. Different reasons have been proposed for this: deletion in the fsr locus point mutation in the gelE gene [36] or loss of the responsible gene as observed in the probiotic strain, Symbioflor [37].
Gelatinase production appeared to be associated with the quantity of biofilm produced by human fecal E. faecalis isolates [22]. In this study, 90% of the fecal isolates were able to produce biofilm, but had no gelatinase activity. These results indicated that gelatinase had a role in the pathogenesis of enterococci, as suggested in another study [35]. Similar to our data, no differences in biofilm production have been observed between gelE+ and gelE- isolates in the pathogenic or fecal isolates [27].
The incidence of hemolysin in our study was much lower than that reported in other studies [1438]. However, similar to other studies, the presence of cyl was not correlated to its phenotypic expression [439]. This lack of cytolysin phenotypic/genotypic congruence might suggest the occurrence of missing genes in the cyl operon [4]. The presence of cytolysin had no significant correlation with biofilm formation. The data reported here are in agreement with some previous studies [28] and in contrast with the results of Tsikrikonis et al [14].
In conclusion, the detection of esp, gelE, and cyl-negative/biofilm formers and esp, gelE, and cyl-positive/non-biofilm formers among the pathogenic and fecal isolates indicated that the esp, gelE and cyl genes in pathogenic and fecal isolates were neither necessary nor sufficient for the production of biofilms by enterococci. Other factors may be involved in this process. Virulence and biofilm formation share a complex relationship through a series of events coordinated through cell-cell communication and mediated by peptides in Gram-positive bacteria. Because biofilm formation is regulated by a complex network of transcriptional factors [40], further investigations are needed to elucidate the relationship between particular virulence genes and biofilm formation.
 XML Download
XML Download