

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Owing to its broad antibacterial spectrum and documented efficacy, piperacillin/tazobactam (TZP), when indicated based on the severity of infection, has been prescribed widely in both community and healthcare settings [12]. Several recent studies regarding its efficacy for treating infections caused by extended-spectrum β-lactamase (ESBL)-producing organisms highlight the usefulness and importance of TZP as broad-spectrum antibiotics in the treatment of serious infections [34].
For a rapid antibacterial effect and the restriction of resistance development, dosing of TZP is important. Usually, the initial recommended dose of TZP is categorized into three groups based on the glomerular filtration rate (GFR), and the maintenance dose is recommended to achieve maximized free time above the minimum inhibitory concentration (Ft>MIC) [56789]. However, the initial dose could be either too high or low for some patients, depending on the patient characteristics, such as renal dysfunction, and critical illness status. In addition, the maintenance dose should be adjusted appropriately using therapeutic drug monitoring (TDM) to improve outcomes, particularly in critically ill patients [10]. Therefore, dosing regimens of TZP need to be individualized and monitored by TDM using data from patient population pharmacokinetics.
Race is one of the important individual characteristics and ethnic differences may affect drug pharmacokinetics or pharmacodynamics [1112]. Several previous studies evaluated the population pharmacokinetics and pharmacodynamics of piperacillin and tazobactam in Korean patients who had burn injuries and renal failure [1314]. However, to our knowledge, no studies have evaluated the population pharmacokinetics in hospitalized Korean patients with infections.
Our institution has performed studies to develop and validate the individualized dosing of important antibiotics in Korean patients [15]. There are fundamental differences in the fat distribution, metabolism, drug transport genetics, and antibiotic clearance (CL) between western and Korean patients. Therefore, in the present study, we aimed to determine the population pharmacokinetics and CL equations of TZP in Korean patients with infections, which could help to develop individualized dosing of TZP based on an understanding of its inter-ethnic differences.
Materials and Methods
1. Study population
From April 2013 to April 2015, patients with acute infections aged over 20 years who had or were expected to have TZP-susceptible pathogens, were enrolled in six university-affiliated hospitals in Korea. The study protocol and informed consent form were approved by the Institutional Review Board of each of the six hospitals that enrolled the study patients. Written informed consent was obtained before enrollment in this study. The following exclusion criteria were used: history of hypersensitivity to beta-lactams; use of drugs known to interact with piperacillin or tazobactam such as vecuronium, heparin, warfarin, methotrexate, and probenecid; and aspartate aminotransferase or alanine aminotransferase exceeding three times the upper limit of the normal range.
2. Study design and dosage regimen
At least four consecutive 2/0.25 g or 4/0.5 g doses of TZP were intravenously infused over 1 h every 8 h to patients with creatinine clearance ≤50 mL/min or creatinine clearance > 50mL/min, respectively. Creatinine clearance (CLcr) was calculated using the Cockroft-Gault formula.
Blood samples from patients at a steady-state were taken pre-dose and at 0 min (immediate), 30 min, and 4-6 h after the fourth infusion. All blood samples were drawn in heparinized tubes, and samples were placed on ice for 0.5–1 h until centrifugation. The plasma samples obtained were separated, promptly aliquoted, and stored at -70°C.
3. Bioanalysis
Concentrations of piperacillin and tazobactam were analyzed using validated liquid chromatography–tandem mass spectrometry (LC–MS/MS), Agilent 1,100 series LC system (Agilent, Wilmington, DE, USA). Piperacillin, tazobactam, and their internal standard (doripenem) were prepared by protein precipitation with 60% acetonitrile. Detection and quantification were performed using a triple quadrupole tandem mass spectrometer with an electrospray ionization interface in the positive and multiple-reaction-monitoring modes. Chromatographic separation of the compounds was accomplished using an Atlantis HILIC column (50 × 2.1 mm, 3 µm; Waters, Milford, MA, USA) with an isocratic elution.
A full validation of the assay was carried out with respect to selectivity, accuracy, precision, recovery, calibration curve, and stability. The calibration curves for piperacillin and tazobactam were linear over ranges of 2.0–500.0 µg/mL and 0.2–50.0 µg/mL, respectively, with coefficients of determination (R2) greater than 0.995 for all.
4. Pharmacokinetic evaluations
PK analysis with a mixed-effects method was performed using NONMEM software (version 7.3; Icon Development Solutions, Ellicott City, MD, USA), employing a first-order conditional estimation with an interaction method throughout the entire modeling process. Model evaluation and selection were based on graphical and statistical methods. Likelihood ratio test results were considered statistically significant if the objective function value (OFV) of nested models decreased more than 3.84 points (chi-square distribution, degree of freedom = 1). Both one- and two-compartment models were tested for the PK model, and linear (first-order) and non-linear (Michaelis-Menten) elimination were investigated. The inter-individual variability of each parameter was described using a log-normal variance model. Additive, proportional, and combined error models were tested to describe residual error. All population pharmacokinetic model processes were equally applied for piperacillin and tazobactam.
Demographic and clinical characteristics such as age, sex, body weight, creatinine clearance using Cockroft-Gault equations (CLcr), blood urea nitrogen, Acute Physiology and Chronic Health Evaluation II (APACHE II) score, and Glasgow Coma Scale (GCS) score were screened as candidate covariates for linear, exponential, and power models. The covariate screening process was performed using visual (parameter versus variable scatterplots/matrix plots) and numerical covariate searching steps. V1 (volume of central compartment) was adjusted for median body weight a priori with a linear relationship with reference to the previous study [16]. During the covariate model-building process, stepwise forward selection and backward elimination were applied.
A non-parametric bootstrap analysis was performed as an internal model evaluation. The final model parameter estimates were compared with the median parameter values and the 2.5–97.5 percentiles of the 1,000 non-parametric bootstrap replicates. The model was also evaluated by visual predictive checks (VPCs) by overlaying observed data points with 5th, 50th, and 95th percentile curves of 2,000 virtual patients simulated from the final model.
Results
1. Subject characteristics
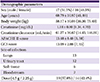
In total, 35 patients completed the study, and plasma samples from volunteers who received all of the planned treatments were analyzed. Data from two patients were excluded for the evaluation, because sampling at the injection site was suspected (concentrations of piperacillin and tazobactam of the two patients were found to be almost 1,000-fold higher than those of other patients). Thus, 33 patients (17 men, 16 women) were included in the population PK analysis. Body weight ranged from 36.30 to 75.40 kg, and CLcr from 14.45 to 146.01 mL/min. Demographic data for participants are shown in Table 1.
Table 1
Demographics of study subjects
2. Population PK model for piperacillin
A two-compartment model with first-order elimination was selected over a one-compartment model which showed a wave pattern in the conditional weighted residual plot suggesting an incorrect structure model. Residual variability was most effectively explained by a proportional error model. The V1 (volume of central compartment) was adjusted for median body weight of 60 kg with a linear relationship. The CLcr was selected as a covariate on CL (clearance of central compartment) with a linear relationship to CL. The CLcr, ranged from 14.45 to 146.01 mL/min, on CL significantly reduced the objective function value (OFV 10.387 decreased) and improved the goodness of fit (GOF). No trends that suggested misspecification in the final model were identified in the GOF plots (Fig. 1). Therefore, the final model was as follows:
Figure 1
Goodness of fit plots for the final pharmacokinetic models for piperacillin (4 figures of the upper panel) and tazobactam (4 figures of the lower panel). The grey line indicates the line of identity; the red line indicates the linear regression line.
CWRES: conditional weighted residual.

Final PK parameter estimates with corresponding relative standard error values and results of the non-parametric bootstrap for piperacillin are summarized in Table 2. The VPC plot in Figure 2 demonstrated the 95% CI and prediction intervals (PI), which adequately described the observed concentrations at each time point with no notable bias.
Table 2
Final estimates of pharmacokinetic parameters for piperacillin and tazobactam
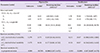
aRelative standard error.
b2.5-97.5 percentile estimated by applying final pharmacokinetic model to 1,000 non-parametric resampled data sets.
CI, confidence interval; CL, clearance; Q, intercompartmental clearance; V1
, volume of central compartment; V2
, volume of peripheral compartment; CV, coefficient of variation
Figure 2
Visual predictive check for the final piperacillin pharmacokinetic model, simulation of 2,000 data sets, using the final pharmacokinetic parameter estimates. Open circles indicate observed concentrations; the red full line indicates the median value; the lower and upper red dotted lines indicate the 2.5th and 97.5th predicted value, respectively.

3. Population PK model for tazobactam
A two-compartment model with first-order elimination was selected. Residual variability was most effectively explained by a proportional error model. Similarly to piperacillin, V1 (volume of central compartment) was adjusted for a median body weight of 60 kg with a linear relationship. CLcr was selected as a covariate on CL (clearance of central compartment) to affect CL linearly. The CLcr on CL significantly reduced the objective function value (OFV 17.736 decreased) and improved the goodness of fit (GOF). Therefore, the final model was as follows:
Final PK parameter estimates with corresponding relative standard error values and results of the non-parametric bootstrap are summarized in Table 2. VPC plots in Figure 2 demonstrated that individual predicted tazobactam concentrations concurred with the observed concentrations without systemic bias.
Discussion
In the present study, we evaluated the population pharmacokinetic analysis of TZP in Korean patients with acute infections. Our results suggested that both piperacillin PK and tazobactam PK were well described by a two-compartment model with first-order elimination, and CLcr on CL was a significant covariate for both piperacillin and tazobactam. Notably, clearance of piperacillin in Korean patients is expected to be lower than that in Caucasians in both normal and lower renal function within the normal body weight range. The proposed equation to estimate CL of piperacillin in Korean patients in this study differed from an equation developed in Caucasians, (1.29 × CLcr + 100) × 60/1,000 (CPL Associates, personal contact). The results suggested that optimized dosing of TZP of Korean patients might be different from that in Caucasians, because of the low CL in Korean patients. We believe that further studies should be performed to validate the individualized dosing of TZP to attain a pharmacokinetic or pharmacodynamic targets in Korean patients.
Individualization and optimization of antibiotic dosing regimens, which become gradually achievable using pharmacokinetics, are particularly important in commonly used antimicrobial agents such as piperacillin and tazobactam [17]. Ethnic differences in the pharmacokinetics of various drugs are widely understood, and it is possible that optimization of piperacillin dosing may be influenced by individual characteristics of different races. However, a paucity of data regarding ethnic differences in pharmacokinetics of piperacillin and tazobactam is available, despite several reports of the population pharmacokinetics of piperacillin and tazobactam [18]. We posit that our present study implies that lower clearances of piperacillin and tazobactam in Korean patients with either normal or lower renal function, compared that with in Caucasians, could enhance the chance of attaining a pharmacokinetic or pharmacodynamic target, even with smaller dosing of piperacillin and tazobactam. The difference in body weight and composition between Korean and Caucasian patients may affect this result, which is supported by results obtained from previous studies that reveal the impact of body composition and body size on pharmacokinetics between different races [1920]. In addition, two recent studies showing that the pharmacokinetics of piperacillin and tazobactam was altered by physiological processes associated with obesity support these results [2122]. However, further studies to determine conclusive explanations for these differences are needed.
There is considerable evidence that efficacy of TZP is influenced by appropriate dosing and mode of administration, as well as the minimal inhibitory concentration of piperacillin [891723]. However, care should be taken to interpret the results, because most of the previous pharmacokinetic studies did not consider the potential impact of dosage regimens on ethnic differences. It would be ideal to calculate the appropriate dose of TZP to achieve the maximized probability of target attainment using stimulation techniques, which could provide individualized dosing regimens and enable an accurate inter-race comparison. In addition, previously reported toxicity of piperacillin associated with impaired renal function should be compared between ethnic groups, because categorizing dosing by the degree of crude renal function may to be too high or low for patients in the same category, according to race [2425].
This study has the following limitations. First, it is a preliminary study to determine the characteristics of piperacillin and tazobactam pharmacokinetics in Korean patients without an efficacy evaluation and validation of dosage regimens. To investigate the ethnic variability, we should calculate the probability of target attainment using population pharmacokinetics in combination with Monte Carlo simulations. Second, the number of patients analyzed in our study was too small to be conclusive and to effectively evaluate the different CL of TZP between races. Therefore, we plan to enroll sufficient patients to confirm and validate individualized dosing of TZP by analyzing clinical outcomes of patients treated with antibiotics from the established equation for drug CL in Korean patients, as well as Monte Carlo simulations.
In conclusion, the PK profiles of TZP at a steady-state in Korean patients with acute infections were well described by two-compartment models with first-order elimination. Clearances of both piperacillin and tazobactam were significantly influenced by creatinine clearance. This model should be validated for the individualized dosing of TZP to attain a pharmacokinetic target in a large number of patients.
 XML Download
XML Download