

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Acute respiratory infection is a major cause of morbidity, hospitalization, and mortality with a worldwide disease burden estimated at 113 million disability-adjusted life years and 3.5 million deaths [1]. Respiratory infection is caused by various pathogens, but approximately 80% of cases are viral [2]. Because respiratory viral infection is characterized by a wide range of similar respiratory symptoms, it is difficult to make an etiologic diagnosis based solely on observable symptoms.
Recently, widespread use of multiplex reverse transcription polymerase chain reaction (RT-PCR)-based methods has greatly improved the diagnostics for respiratory viral infections [3]. It provides a more accurate diagnosis of causative pathogens and a better understanding of the etiology of infection. However, most epidemiologic investigations of respiratory virus infections have focused on children, and few studies have been conducted with an adult population. Yet, understanding the etiologies and clinical profiles of respiratory viral infections are essential for improving preventive and therapeutic strategies.
Here, we report a retrospective observational study that describes the viral etiologies of acute respiratory infections in children and adults and the clinical features of respiratory viral infections for adults.
Materials and Methods
1. Study population and data collection
We investigated patients who were hospitalized at Korea University Guro Hospital (KUGH) due to acute febrile respiratory illness between July 2009 and April 2012. For these patients, we used the hospital's microbiologic database to identify those who had one or more respiratory samples sent to the hospital's diagnostic laboratory for testing with a multiple real-time PCR assay specific for detecting a panel of viruses as part of their routine workup. Besides the availability of real-time PCR virus detection data, the inclusion criteria for this study were as follows: (1) acute febrile illness (≥ 38.0℃), (2) a diagnosis of respiratory infection, including upper respiratory infection, bronchitis, bronchiolitis, bronchopneumonia, or pneumonia, and (3) hospitalization. Duplicate samples positive for virus and collected from the same patient within a week were excluded from analysis. Co-detections were counted as separate cases. Nosocomial infections were excluded by identifying and omitting cases in which respiratory symptoms developed ≥ 2 days after admission. The isolation rate for each respiratory virus was defined as the ratio of the number of patients showing the presence of the given virus divided by the total number of specimens submitted for multiple real-time PCR assay during the study period. Each isolation rate was analyzed monthly. Patients were divided into two groups: children < 15 years old and adults > 19 years old. Clinical data for adults were obtained from medical records. Data included demographic characteristics, presenting symptoms, diagnosis at admission, length of hospital stay, need for intensive care unit (ICU) care, and mortality.
2. Laboratory procedures
Most of the respiratory samples were collected by nasopharyngeal swab, nasopharyngeal aspiration, or throat swab. Total nucleic acids were extracted from 200 mm3 of each specimen using virus transport medium (VTM). The presence of influenza virus (IFA/IFB), respiratory syncytial virus (RSV A, RSV B), parainfluenza virus (PIV 1-4), adenovirus (AdV), human rhinovirus (hRV), human metapneumovirus (hMPV), human coronavirus (hCoV-229E, hCoV-OC43), human bocavirus (hBoV), and enterovirus (EV) was determined using the Seeplex ® RV15 real-time PCR assay (Seegene, Inc., Seoul, Korea). The Seeplex RV15 assay kit contained A and B sets of primers designed from conserved regions of genetic sequences for the 15 respiratory viruses mentioned above. An initial pre-PCR step of 94℃ for 15 minutes was performed, and this was followed by a total of 35 PCR cycles according to manufacturer's instructions. VTM alone was used as a negative control. PCR products were analyzed by electrophoresis in 2% agarose gel containing ethidium bromide. The types of respiratory virus were identified by comparison with the reference band size provided by the manufacturer.
3. Statistical analyses
For categorical variables and continuous variables, the chi-squared test and t-test were performed, respectively, to compare the characteristics of adult patients with solitary viral detection and bacterial co-detection. Categorical variables included respiratory symptoms (fever, congestion/rhinorrhea, cough, sputum, nausea/vomiting/diarrhea), comorbidity, presence of lower respiratory infection, and clinical outcomes such as ICU admission and mortality. Continuous variables included mean length of hospital stay. A P-value < 0.05 (two-tailed) was considered significant. These analyses were conducted using SPSS 18.0 for Windows (SPSS Korea, Seoul, Korea).
Results
1. Distribution of respiratory viruses for each age group
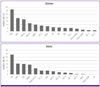
During the study period, respiratory samples obtained during 3,865 clinical episodes involving children were tested for the presence of virus. The median patient age was 27 months, with 57.3% of participants being 1-5 years of age. Among the specimens, 2,800 (72.4%) were positive for ≥ 1 respiratory virus (Table 1). The most commonly identified pathogens were hRV (889, 31.8%), AdV (537, 19.2%), RSV A (486, 17.4%), RSV B (328, 11.7%), and hMPV (273, 9.8%). PIVs were detected in 11.8% of specimens, with the PIV3 strain representing the majority (8.4%). The detection rates for other viruses are shown in Figure 1.
In contrast to children, a total of 763 specimens were obtained from adults and 205 (26.9%) were positive for ≥ 1 respiratory virus (Table 1). As shown in Figure 1, IFA had the highest detection rate (59, 28.5%) followed by hRV (32, 15.5%), IFB (31, 15.0%), and hMPV (29, 14.0%). hCoV-229E and EV were not detected in adults during the study period. Similar to children, PIV3 was the dominant strain detected among PIV viruses.
2. Seasonal distribution of IFA, IFB, RSV A, RSV B, PIV 1-4, AdV, and hMPV
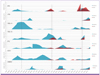
Many of the detected respiratory viruses varied in a season-dependent manner during the study period (Fig. 2). hCoV-229E, hCoV-OC43, hBoV, and EV were excluded from this analysis because the isolated numbers were too low. IFA, IFB, RSV A, RSV B, and hMPV exhibited strong seasonal patterns. IFA peaks were observed in winter (November to January), and IFB was active in spring (January to March). RSV A and RSV B showed a peak of increased winter detection (November to February) in an apparent biennial pattern. PIV and AdV showed no discernible seasonal peaks and generally even detection across the study period. Despite lower detection, hMPV showed a seasonal pattern (March to May) similar that of IFB. Similar circulating patterns were observed for children and adults, especially for IFA, IFB, RSV A, RSV B, and hMPV.
3. Clinical profiles associated with IFA, IFB, RSV A, RSV B, PIV1-4, AdV, hMPV, hRV, and hCoV-OC43
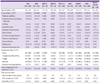
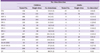
The clinical characteristics of adult patients with IFA, IFB, RSV A, RSV B, PIV1-4, AdV, hMPV, and hRV infection are summarized in Table 2. The patients with hRV, RSV B, and AdV tended to be younger, and those infected with RSV A and hMPV tended to be older. Comorbidities were more common in patients with IFB, RSV A, RSV B, PIV, and hRV infection. The common comorbidities were diabetes mellitus, chronic renal disease, and malignancy. Patients presented with similar respiratory symptoms. However, nasal congestion and rhinorrhea were more common with hRV (82.8%) and hCoV-OC43 (69.2%) infection. Cough was less common with RSV A infection (80%) compared to the others. Lower respiratory infection was found in about 50% of patients for most viruses, although the percentages were somewhat higher for hMPV (69%) and PIV 1-4 (66.7%). The patients with RSV A infection tended to stay longer in hospital, enter the intensive care unit (ICU), and die more frequently.
4. Co-detection of respiratory viruses
Among the positive cases, multiple virus detection (≥ 2 viruses) was observed in 868 children (22.4%) and 11 adults (2.0%). Dual and triple virus detection was present in 677 (17.5%) and 165 (3.3%) children, respectively, and 10 (1.3%) and 1 (0.2%) adult(s), respectively. Four or five viruses were simultaneously detected in 26 (0.7%) children, but this level of co-infection was not observed in our adult population. The frequencies with which individual pathogens were identified as solitary and co-detections are shown at Table 3. IFB, RSV A, and RSV B were more likely to be identified as solitary pathogens, whereas hRV, EV, and hMPV were more likely to be identified as co-infections in children. The number of total co-detections was too low in adults to warrant further analysis. RSV A and RSV B were the viruses most often detected concurrently with other respiratory viruses in adults.
5. Clinical profiles associated with bacterial co-detection
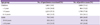
Among the 166 adult patients with IFA, IFB, RSV A, RSV B, PIV1-4, AdV, hMPV, hRV, and hCoV-OC43 infection, bacterial sputum culture was performed for 140 patients (84.3%). For these patients, bacteria were isolated in 44 cases (26.5%). Bacterial isolation rates and co-detected species for each virus are shown in Table 4. Staphylococcus aureus and Streptococcus pneumoniae were the most frequent bacterial isolates. There were no symptomatic differences between bacterial co-detection cases and solitary viral detection cases. Cases with bacterial co-detection were more likely to have lower respiratory tract involvement, longer hospital stay, and higher mortality (Table 5).
Discussion
Respiratory infection is one of the most common human infections. Among the causative agents, viruses are the major pathogen of acute respiratory infection. This study describes the age-dependent distribution, potential etiologies, and seasonal patterns of acute viral respiratory infection among hospitalized children and adults in Korea. In addition, this study focused on the clinical profiles of common viral infection (IFA/IFB, RSV, PIV, AdV, hMPV, hRV, and hCoV-OC43) in adult patients.
A microbiologic database was reviewed to identify the prevalence of 15 viruses in the hospitalized children and adults with acute respiratory infection. Compared to the respiratory virus isolation rate in children (72.4%), the isolation rate was low in adults (26.9%). It should be noted that the isolation rate in adults may have been underestimated because, in general, respiratory specimens were collected through nasopharynx/throat swabs in adults, whereas nasopharyngeal suction was used in children and adolescents. In addition, adults may have already acquired some level of immunity through previous exposure to the same respiratory viruses, so viral shedding may not persist as long in adults as in children.
Viral agents were detected in 26.9% of the adult patients, with the most common viruses being hRV, IFA, IFB, and hMPV. In comparison, hRV had the highest isolation rate, followed by AdV, RSV A/B, and hMPV, in children. Thus, different respiratory viruses should be considered depending on the patient's age when a clinically relevant respiratory infection is suspected. Our findings are consistent with other studies focused on adult patients [4, 5, 6]. However, the frequencies of detection for each virus were different. These differences likely originated from distinct study designs and patient populations, and seasonal variations during the study periods. In the present study, hRV and IFA/IFB were major pathogens associated with hospitalization of both children and adults. Although influenza virus is well recognized as an important cause of hospitalization, the roles of other respiratory viruses are not well defined. It had been generally acknowledged, except for severely immunocompromised hosts, that hRV was not commonly associated with severe illness resulting in hospitalization. However, with the implementation of molecular diagnostic techniques, the human hRV is now being recognized as one of the common causes of hospital admission [4, 5, 6]. Although serious sequelae are infrequent, hRV should be considered in the virologic diagnosis of severe respiratory infections [7, 8].
Simultaneous detection of two or more respiratory viruses in adults occurred less frequently than in children. Two or more pathogens were detected simultaneously in 2.0% of the adults; RSV A and RSV B were frequently co-detected. The clinical significance of co-infection remains uncertain. Co-detection could indicate a pathogenesis that requires interaction of the co-detected respiratory viruses. Alternatively, co-detection could merely reflect residual viral shedding from a previous infection or incidental virus that is commonly found in the upper airways with unclear clinical significance [9]. A previous study of infants showed that co-infections of RSV and other viruses caused a higher incidence of fever and longer duration of hospitalization compared to solitary RSV infection [10]. However, in some studies, no clinical differences were reported [11, 12]. In this study, the number of cases was too small to compare the clinical outcomes. Further studies are required to understand the potential respiratory virus interactions and the clinical differences between single and concurrent multiple infections.
It has been demonstrated that viral infection can enhance bacterial adherence and immune-mediated interactions [13]. The occurrence of staphylococcal and pneumococcal pneumonia complicating Spanish influenza pandemics is well known. Recent pandemic influenza H1N1 2009 showed overall rates of bacterial co-detection of 20%-24% [14]. Our study demonstrated a similar prevalence of bacterial co-detection of 26.5%. S. pneumonia and S. aureus are commonly recognized etiological agents, and data in this study are consistent with this [15]. Despite no apparent difference in clinical symptoms, lower respiratory tract involvement, length of hospital stay, and mortality were more common in cases with bacterial co-detection. This information may help with the decision to use an antibiotic.
Data on the seasonal prevalence of each respiratory virus would be useful for diagnosis and planning control strategies. In this study, we found that IFA/IFB, RSV A, RSV B, and hMNV exhibited strong seasonal patterns in Korea. Influenza prevalence peaked during the winter, and RSV's yearly epidemic occurred primarily in and around winter. hMPV typically peaked in the spring, slightly later than RSV. In the cases of IFA/IFB, RSV A/B, and hMPV, similar seasonal patterns were observed in children and adults. While it is not clear whether epidemics in children lead to adult epidemics, virus prevalence information for children may be useful to predict subsequent epidemics in adults.
Consistent with previous studies, adult patients infected with IFA/IFB, RSV A/B, PIV1-4, AdV, hMPV, hRV, and hCoV-OC43 presented with different respiratory symptoms, comorbidities, and rates of lower respiratory tract infection[16, 17]. However, these findings might not be particularly useful for rapidly and accurately identifying the etiologic virus. Clinical diagnosis based on the patient's age and clinical features and on concurrent epidemic information should be made with discretion. Rapid and highly accurate diagnostic tests such as real-time PCR assays should be considered in severe and complicated patients.
This study had several limitations. First, the decision to admit patients and take respiratory samples was made at the discretion of the attending physician. Second, real-time PCR may be overly sensitive and pathogen detection may not accurately reflect true respiratory infection. Third, not all specimens were tested for the presence of viruses, which likely would have increased the number of pathogens identified. Fourth, over the study period, the number of real-time PCR analyses were gradually increased, so the number of submitted samples analyzed in the early part of the study was small. Thus, more recent analysis results are likely to be over represented. Finally, the etiology of respiratory viral infection appears to differ according to the patient's age, especially for children. This made it difficult to conduct meaningful subgroup analyses stratified by age due to the reduced number of child patients per subgroup.
In conclusion, the etiologic virus of an acute respiratory infection can be cautiously inferred based on a patient's age and clinical features and concurrent epidemic information. Large-scale prospective surveillance studies are required to provide more accurate information about respiratory viral infection etiology, which could favorably influence clinical outcomes.


 XML Download
XML Download