

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Emphysematous prostatitis is a rare condition that is characterized by gas and abscess accumulation in the prostate [1-5]. There have been several reports of this uncommon but serious disease. This disease entity requires special attention by physicians due to its nonspecific presentation such as dysuria, frequency, urgency, fever, acute urinary retention and/or perineal pain [1-5]. Some authors have demonstrated that this condition is an uncommon, but relatively serious disease with high mortality and morbidity [1-5]. We report herein on a case of emphysematous prostatitis combined with liver abscess caused by K. pneumoniae.
Case report
A 55-year-old man visited the emergency department due to a 3-day history of urinary retension with a febrile sensation.
He had not traveled anywhere for the past 6 months, and he denied alcohol consumption and smoking. He complained of voiding difficulty and vague lower abdominal discomfort.
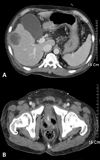
The day before this presentation, he visited a private clinic and was referred to a general hospital for further evaluation. He underwent an abdominopelvic computed tomography (CT) scan, which revealed a single lesion in the right lobe of the liver and a normal prostate (Fig. 1A and Fig. 1B). The clinician advised this patient to be admitted for further evaluation of the lesion, but he refused. When he visited our ER, his bladder was remarkably distended and urinary catheterization was quickly performed.
He had a 1-year history of chronic hepatitis C with liver cirrhosis (Child-Purr class B) and a 10-year history of uncontrolled diabetes mellitus.
On the physical examination, no specific signs were checked. His blood pressure was 160/90 mmHg, the body temperature was 38.4℃, the pulse rate was 130 per minute and the respiratory rate was 20 per minute. The initial chest radiography and electrocardiography were normal. The laboratory tests showed a WBC: 9,800/mm3, hemoglobin: 11.4 g/dL, platelet: 122,000/mm3, ESR: 61, CRP: 98.1 mg/L, BUN: 23 mg/dL, serum creatinine: 0.8 mg/dL, total proteinL: 6.6 g/d, serum albumin: 2.3 g/dL, serum AST/ALT: 42/33 IU/L, random blood glucose: 382 mg/dL. The random urine pH: 5.0, the specific gravity: 1.025. Urine microscopy exhibited that the RBCs and WBCs were each 0-1/HPF. Blood and urine cultures were performed twice and levofloxacin 500 mg/d was started intravenously.
On the third hospital day, his blood pressure was 80/50 mmHg, the body temperature was 36.8℃, the pulse rate was 128 per minute and the respiratory rate was 22 per minute. The urologist transferred this patient to the infectious disease clinic for the management of septic shock. The kidneys-ureters bladder (KUB) X-ray showed pockets of air-accumulation in the lower pelvic cavity, and the abdominopelvic CT with dynamic contrast enhancement taken on the third day showed a 5-cm liver abscess with an emphysematous prostate (Fig. 2, Fig. 3A and Fig. 3B). Levofloxacin was changed to metronidazole 500 mg q.i.d. and cefotaxime 2 g t.i.d. Ultrasound-guided liver abscess aspiration yielded about 17 mL of yellow material, which was then cultured. We consulted with a urologist about drainage of the emphysematous prostatitis.
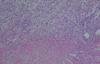
On the sixth day, the urologist performed transurethral resection and drainage under spinal anesthesia. Cribriform prostatic tissue, gas and a pus-like discharge mixed with blood were observed by resectoscopy. Some of the infected prostatic tissue was cultured. However, the postoperative bleeding control failed and the patient's hypovolemic shock persisted, which then provoked multiorgan failure. An intravenous inotropic agent and intubation with mechanical ventilation were applied at the intensive care unit. Continuous renal replacement therapy was performed. Despite the efforts, the patient died on the 11th hospital day. K. pneumoniae was cultured from the liver abscess aspirate and the two samples of blood and prostatic tissue. Isolated K. pneumoniae was sensitive to both levofloxacin and cefotaxime. Histopathologically, necrotic tissue and many inflammatory cells were noticed (Fig. 4).
Discussion
Emphysematous prostatitis is a serious disease, but it is hard to diagnose because of its rarity and nonspecific symptoms [1-5]. A delayed diagnosis can cause high mortality and morbidity, so a prompt clinical diagnosis of this condition is essential [1-5]. The majority of patients present in their fifth or sixth decade of life and they have other predisposing factors including diabetes mellitus, liver cirrhosis, intravesical obstruction and prior genitourinary tract instrumentation and bladder catheterization [1-5]. This disease can be diagnosed at an early stage with advanced diagnostic modalities such as ultrasound, CT or MRI [1-5]. Appropriate antibiotics with early incision and drainage may result in favorable outcomes. In our case, emphysematous prostatitis was present along with a liver abscess due to K. pneumoniae.
K. pneumoniae has been reported to be the most common pathogen causing liver abscess in Korea [6, 7]. The incidence of K. pneumoniae infection increases in immunocompromised conditions, such as diabetes mellitus, alcoholism, malignancy, hepatobiliary disease, chronic obstructive pulmonary disease, glucocorticoid therapy and renal failure [6-14]. In our case, the patient had several risk factors for K. pneumoniae infections, including diabetes mellitus and liver cirrhosis associated with chronic hepatitis C.
In a few cases, K. pneumoniae liver abscess has been associated with metastatic infection at other sites [7, 8, 10-18]. Some investigators have reported that a minority of patients with Klebsiella liver abscess, and mostly from Taiwan, develop metastatic infection as manifested by endophthalmitis, uveitis, pneumonia, pulmonary abscess, pulmonary emboli, pulmonary abscess, pleural empyema, peritonitis, subcutaneous abscess, deep neck infection involving the mediastinum, splenic abscess, brain abscess, purulent meningitis, epidural abscess, renal abscess, prostate abscess, osteomyelitis, pyogenic arthritis and psoas abscess [7, 8, 10-18]. This disease entity is called invasive liver abscess syndrome, which is caused by the hypervirulent K. pneumoniae subtypes [9, 11-14, 16, 17]. Recent studies have shown that the mucoviscosity-associated gene A (magA) and regulator of mucoid phenotype A (rmpA) are associated with this syndrome [9, 12-14, 17]. However, we could not ascertain which phenotype and genotype produced invasive K. pneumoniae syndrome in our case.
Emphysematous prostatitis is a rare and serious condition [1-5]. There have been some reports about emphysematous prostatitis due to K. pneumoniae, but emphysematous prostatitis with invasive liver abscess syndrome has not been previously reported. We present here the first case of emphysematous prostatitis that was combined with liver abscess caused by K. pneumoniae.


 XML Download
XML Download