

This article has been corrected. See "ERRATUM: Risk Factors and Prognosis for Persistent Candidemia without Catheter Colonization" in Volume 44 on page 44.
 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Background
Candidemia is one of the most common causes of nosocomial bloodstream infection, and increases the morbidity and mortality rate of seriously ill patients. We evaluated the risk factors and outcomes associated with persistent candidemia without catheter colonization (non-catheter related candidemia) and compared them with those of non-persistent candidemia.
Materials and Methods
A retrospective case-control study was performed to identify risk factors for, and outcomes of, persistent candidemia. All adults who experienced candidemia in a university-affiliated hospital in Korea between January 2005 and December 2009 were included.
Patients with catheter colonization were excluded. Persistent candidemia was defined as the occurrence of candidemia in a patient receiving at least 3 days of systemic antifungal agents prior to the second positive blood culture.
Results
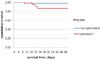
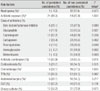
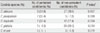
Of 605 adult patients with candidemia, 104 (17.2%) patients had persistent candidemia and 23 (3.8%) patients were free of catheter colonization. There were no statistically significant differences in baseline characteristics between patients with persistent and non-persistent candidemia. In univariate analysis, less use of metronidazole, glycopeptide, fluoroquinolone, and aminoglycoside, and presence of Candida parapsilosis were significantly associated with persistent candidemia. In multivariate analysis, less use of metronidazole was an independent factor associated with persistent candidemia. The candidemia related mortality was insignificantly (P=0.094) higher in persistent candidemia than non-persistent candidemia.
Conclusions
Persistent candidemia can occur without catheterization. Patterns of antibiotic use could be associated with the occurrence of persistent candidemia, and prognosis of persistent candidemia seems to be worse than non-persistent candidemia. Further studies for persistent candidemia should be performed.
Figures and Tables



References
1. Hidron AI, Edwards JR, Patel J, Horan TC, Sievert DM, Pollock DA, Fridkin SK. National Healthcare Safety Network Team. Participating National Healthcare Safety Network Facilities. NHSN annual update: antimicrobial-resistant pathogens associated with healthcare-associated infections: annual summary of data reported to the National Healthcare Safety Network at the Centers for Disease Control and Prevention, 2006-2007. Infect Control Hosp Epidemiol. 2008. 29:996–1011.

2. Kwak YG, Cho YK, Kim JY, Lee SO, Kim HY, Kim YK, Park ES, Jin HY, Choi HJ, Jeong SY, Kim ES, Ki HK, Kim SR, Lee JY, Hong HK, Kim S, Uh Y, Lee YS, Oh HB, Kim EC. Korean nosocomial infections surveillance system, intensive care unit module report: data summary from July 2008 through June 2009 and analysis of 3-year results. Korean J Nosocomial Infect Control. 2010. 15:14–25.
3. Pfaller MA, Moet GJ, Messer SA, Jones RN, Castanheira M. Candida bloodstream infections: comparison of species distributions and antifungal resistance patterns in community-onset and nosocomial isolates in the SENTRY Antimicrobial Surveillance Program, 2008-2009. Antimicrob Agents Chemother. 2011. 55:561–566.
4. Pfaller MA, Moet GJ, Messer SA, Jones RN, Castanheira M. Geographic variations in species distribution and echinocandin and azole antifungal resistance rates among Candida bloodstream infection isolates: report from the SENTRY Antimicrobial Surveillance Program (2008 to 2009). J Clin Microbiol. 2011. 49:396–399.
5. Uzun O, Ascioglu S, Anaissie EJ, Rex JH. Risk factors and predictors of outcome in patients with cancer and breakthrough candidemia. Clin Infect Dis. 2001. 32:1713–1717.
6. Chung JW, Lee SO, Choi SH, Woo JH, Ryu J, Kim YS, Kim NJ. Risk factors and outcome for breakthrough candidaemia in patients with cancer. Mycoses. 2006. 49:114–118.
7. Kontoyiannis DP, Vaziri I, Hanna HA, Boktour M, Thornby J, Hachem R, Bodey GP, Raad II. Risk Factors for Candida tropicalis fungemia in patients with cancer. Clin Infect Dis. 2001. 33:1676–1681.
8. Pasqualotto AC, Nedel WL, Machado TS, Severo LC. Risk factors and outcome for nosocomial breakthrough candidaemia. J Infect. 2006. 52:216–222.
9. Nucci M, Colombo AL. Risk factors for breakthrough candidemia. Eur J Clin Microbiol Infect Dis. 2002. 21:209–211.
10. Lee I, Fishman NO, Zaoutis TE, Morales KH, Weiner MG, Synnestvedt M, Nachamkin I, Lautenbach E. Risk factors for fluconazole-resistant Candida glabrata bloodstream infections. Arch Intern Med. 2009. 169:379–383.
11. Lin MY, Carmeli Y, Zumsteg J, Flores EL, Tolentino J, Sreeramoju P, Weber SG. Prior antimicrobial therapy and risk for hospital-acquired Candida glabrata and Candida krusei fungemia: a case-case-control study. Antimicrob Agents Chemother. 2005. 49:4555–4560.
12. Cury AE, Hirschfeld MP. Interactions between amphotericin B and nitroimidazoles against Candida albicans. Mycoses. 1997. 40:187–192.
13. Chang MR, Cury AE. Amphotericin B-metronidazole combination against Candida spp. Rev Iberoam Micol. 1998. 15:78–80.
14. Nguyen MH, Peacock JE Jr, Tanner DC, Morris AJ, Nguyen ML, Snydman DR, Wagener MM, Yu VL. Therapeutic approaches in patients with candidemia. Evaluation in a multicenter, prospective, observational study. Arch Intern Med. 1995. 155:2429–2435.
15. Nucci M, Colombo AL, Silveira F, Richtmann R, Salomão R, Branchini ML, Spector N. Risk factors for death in patients with candidemia. Infect Control Hosp Epidemiol. 1998. 19:846–850.
 XML Download
XML Download