

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Bortezomib (Velcade), formerly known as PS-341 (Millennium Pharmaceuticals, Inc, Cambridge, Mass), is a novel selective and reversible proteasome inhibitor (1,2). This drug has been shown to produce significant responses in one third of patients with progressive relapsed and refractory multiple myeloma (MM) (3). Antitumor activity of bortezomib against MM was found to block proteasome degradation of IκB, an inhibitor of NF-κB (2). NF-kB induces cytoprotective gene expression in hepatocytes attenuating liver injury (4). There have been few reports regarding severe liver toxicity caused by bortezomib treatment in MM, aside from reports of transient enzyme elevations (5). Herein, we present the case of a patient with MM, who developed severe hepatitis after starting bortezomib therapy. For this patient, thalidomide-containing therapy followed by planned high-dose melphalan with stem cell support was successfully performed.
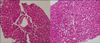
A 52-year-old man was diagnosed as having stage IIIB kappa light chain MM in January 2010. The patient was diagnosed with MM based on a history of anemia, hypercalcemia, and kidney injury associated with elevated concentrations of serum kappa-free light chain. A bone marrow biopsy revealed 71% plasma cells with abnormal cytogenetics, such as t(11:14) and chromosome 13 deletion. Induction therapy was started using high dose dexamethasone for 2 cycles, but the patient's disease continued to progress through 2 courses of high dose dexamethasone. The patient began bortezomib therapy at the usual schedule dosing of 1.3 mg/m2 on days 1, 4, 8, and 11, every 3 weeks. On day 8, the patient was admitted to the hospital with marked fatigue and epigastric discomfort. On admission, there was a severe increase in liver enzyme levels (aspartate aminotransferase [AST] level, 1,856 U/L (normal <40); alanine aminotransferase [ALT] level, 2,865 U/L (normal <40); alkaline phosphatase level 510 U/L (normal <125); and γ-glutamyl transpeptidase level, 139 U/L (normal <40). Bilirubin levels were found to be normal during bortezomib therapy. His serologic tests for hepatitis B and C virus were negative. In addition, cytomegalovirus serology was negative. Serum free kappa light chains were noticeably reduced. The results of an ultrasonogram and a CT scan of his liver were normal. The patient had no known history of liver disease or alcohol abuse. A percutaneous hepatic biopsy of the lesions was performed, and as shown in Fig. 1, histology showed severe lobular activity (more than 10 necrosis per 10× objective field, or confluent necrosis). We considered the cause of elevations of liver enzyme levels as toxic hepatitis. His baseline liver functions were normal. The increase in liver enzyme levels occurred after the second dose of bortezomib was administered and after this peak was reached, the patient was discontinued from bortezomib therapy and his liver enzyme levels quickly decreased to practically normal values after 2 weeks (Fig. 2). The normalization of liver enzyme levels following discontinuation of bortezomib suggests that this drug was the cause of the severe hepatitis. After liver toxicity was resolved, the patient was switched to thalidomide (200 mg/day) therapy with a concomitant high dose of dexamethasone; his AST and ALT levels remained in the baseline ranges during the 3-month induction treatment period. After receiving 3 cycles over a 3-month period, the patient had clearance of serum kappa free light chain and no plasma cells on repeat bone marrow biopsy. An elective autologous stem cell transplant (ASCT) with melphalan (200 mg/m2) conditioning was performed without immediate complications. Maintenance treatment with thalidomide (100 mg/day) was started 2 months after ASCT.
The toxicity of bortezomib is manageable, and toxic effects include gastrointestinal symptoms, neuropathic pain, peripheral neuropathy, and thrombocytopenia (5). In preclinical toxicity studies, bortezomib-related liver changes were present, but the liver was not considered an important target organ of toxicity with the use of this medication. Thus, bortezomib-related liver changes included increases in liver weight due to hepatocellular hypertrophy, vacuolization, and pigment deposition in hepatocytes (5). A completely reversible and severe increase in liver enzyme levels within the peak 3 days after the second dose of bortezomib, without severe hepatic damage associated with infection or hypotension, strongly suggests that this drug was the cause of the liver injury. Another previously-reported case exhibited a similar pattern of bortezomib-related hepatotoxicity occurrence (5). In that case, liver enzyme levels were increased with a peak at 3 days after the second dose of bortezomib was administered. In other words, the finding that a peak in liver enzyme levels was observed in both cases might suggest that the second dose of the drug triggered severe liver toxicity.
Our patient was able to be treated successfully with thalidomide-containing regimens. Although it has been reported that elevated liver enzymes may occur in some patients receiving thalidomide (6), the liver enzyme levels remained normal in this patient, suggesting that there is no cross hepatotoxicity between proteasome inhibitors and immunomodulatory drugs. Drug-induced hepatitis may show different types of liver damage. In our patient, the pathologic damage was observed predominantly in lobular areas, with minimal lesions, rather than in periportal areas. Although severe hepatotoxicity due to bortezomib is relatively rare compared to other drugs, the possibility of acute drug-induced hepatitis must be considered, and a liver biopsy should be considered whenever treatment with this medication begins to impact patient management.

 XML Download
XML Download