

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Cubital tunnel syndrome is the most common compressive ulnar neuropathy in the upper extremities. If conservative treatment fails, operative treatment is indicated. Several techniques are used to treat this condition, including open12 or endoscopic34 simple decompression; subcutaneous,567 intramuscular, 8 or submuscular29 anterior transposition; and medial epicondylectomy.61011 Among them, anterior transposition of the ulnar nerve is the most commonly used procedure for operative treatment of cubital tunnel syndrome.1213 This procedure relieves dynamic ulnar nerve compression that occurs with elbow flexion by transposing the ulnar nerve anterior to the medial epicondyle.14 However, extensive dissection is required to transpose the ulnar nerve, which may compromise the vascularity of the nerve.15 Based on this concept, simple decompression of the ulnar nerve via open or endoscopic techniques have gained popularity.
Another issue that is pertinent to choosing an appropriate surgical technique is ulnar nerve instability while moving the elbow, which occurs in patients with cubital tunnel syndrome. A meta-analysis study reported no differences in nerve conduction velocities and clinical outcomes after performing simple decompression and ulnar nerve transposition for patients with idiopathic cubital tunnel syndrome.15 However, two of the four randomized studies that were analyzed excluded patients with nerve subluxation.1617 In contrast, Bimmler and Meyer18 reported better clinical outcomes in patients with ulnar nerve instability following anterior transposition than after simple decompression. Thus, it is unclear which procedure is better in patients with ulnar nerve instability. In 2011, Keith and Wollstein19 reported excellent clinical outcomes after their tailored approach using a conventional incision in their retrospective study; their approach involved simple decompression in patients without ulnar nerve instability and anterior subcutaneous transposition in patients with nerve instability based on intra-operative ulnar nerve stability assessment. However, this study had a relatively small sample size and non-standardized outcome measures.
As minimally invasive procedures have become popular, simple decompression of the ulnar nerve has been conducted using a minimal incision with satisfactory clinical outcomes.20 Since 2010, we have performed a tailored surgical approach in patients with cubital tunnel syndrome based on an intra-operative ulnar nerve stability test, performing simple decompression in patients without ulnar nerve instability and anterior subcutaneous transposition in patients with nerve instability.
We hypothesized that 1) a surgical decision on whether to perform simple decompression or anterior ulnar nerve transposition based on ulnar nerve stability after making a minimal incision would be effective at postoperative 2 years in a cohort of patients with cubital tunnel syndrome and that 2) certain factors assessed using disabilities of arm, shoulder and hand (DASH) scores could be used to determine the clinical outcome at postoperative 2 years.
MATERIALS AND METHODS
This study was approved by our Institutional Review Board, and all patients provided informed consent before participation. Inclusion criteria included all male and female patients of at least 18 years of age with clinically and electrodiagnostically confirmed cubital tunnel syndrome. Electrodiagnostic studies were conducted and interpreted by a professional rehabilitation doctor at our institution.
From March 2010 to December 2012, 69 consecutive patients with cubital tunnel syndrome awaiting operative treatment were enrolled in the study. We recommended operative treatment for patients with significant weakness on presentation as well as for those with clinical symptoms of tingling, pain, or weakness after at least 2 months of conservative treatment with night splinting and tendon gliding exercises. Exclusion criteria included electrodiagnostically silent cubital tunnel syndrome, cubitus valgus, osseous canal deformity from previous trauma or osteophytes of the elbow joint, previous surgery for cubital tunnel syndrome, associated cervical radiculopathy, carpal tunnel syndrome, ulnar tunnel syndrome, thoracic outlet syndrome, diabetes mellitus, hypothyroidism, arthritis, Burger's disease, cognitive impairment affecting the ability to complete questionnaires, worker's compensation issues, patient refusal to participate in this study, and a follow-up period less than 24 months.
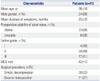
Based on these criteria, two patients with electrodiagnostically silent cubital tunnel syndrome, three patients with cubitus valgus, four patients with elbow osteoarthritis, two patients requiring revision surgery, four patients with one of the associated diseases mentioned above, two patients receiving worker's compensation, and three patients who declined to participate in this study were excluded. Four patients were lost to follow-up. Consequently, 24 patients were excluded, and 41 patients were available for the study. Among our study population, eight patients had bilateral cubital tunnel syndrome. Of these patients, we analyzed only the dominant extremity. The patients consisted of 24 men and 17 women with a mean age of 36 years (range, 19–68 years) at the time of surgery (Table 1). The minimum follow-up was 24 months (mean 36±9 months). Dellon staging was applied to grade the preoperative severity of ulnar neuropathy.20 According to this staging system, patients with intermittent paresthesia and subjective weakness were classified as having mild ulnar nerve compression (grade I). Patients who had moderate compression showed intermittent paresthesia and measurable weakness in pinch and grip strength (grade II). Patients with persistent paresthesia, abnormal two-point discrimination, and measurable weakness in pinch and grip strength with intrinsic atrophy were classified as having severe compression (grade III). All patients underwent preoperative motor nerve conduction tests and electromyography that showed compression of the nerve within the elbow segment. The mean motor nerve conduction velocity at the elbow segment was 43 m/s. According to the Dellon staging system,21 four patients were rated as grade I, 20 as grade II, and the remaining 17 as grade III (Table 1).
An independent observer (BRK) blinded to the method of operation performed the preoperative and postoperative assessments. Each patient was assessed for grip and pinch strength and two-point discrimination and completed the DASH survey preoperatively and at two years after the operation.22 Pinch and grip strength were measured using baseline hydraulic pinch and grip dynamometers. The clinical outcome at two years after the operation was based on the Bishop rating system, which assessed subjective and objective parameters.9 Subjective parameters included severity of residual symptoms (asymptomatic, 3; mild, 2; moderate, 1; severe, 0), subjective improvement from the preoperative period (better, 2; unchanged, 1; worse, 0), and preoperative and postoperative work status (working previous job, 2; changed job, 1; not working, 0). Objective parameters included grip strength relative to the normal side (80% or more, 1; less than 80%, 0) and sensory measurement of static two-point discrimination (≤6 mm, 1; >6 mm, 0). The score was defined as excellent (8 to 9), good (5 to 7), fair (3 to 4), and poor (0 to 2).
Surgical technique
Under general anesthesia, the patient was placed in a supine position with the affected arm supported by a hand table and sterilely prepped and draped. After exsanguination of the limb with a sterile tourniquet, the shoulder was abducted to 90 degrees with slight external rotation, and the medial epicondyle and olecranon were marked. A 2.5-cm longitudinal skin incision was made between the medial epicondyle and the olecranon. The subcutaneous tissues were then gently and carefully separated with dissecting scissors. With the help of mini retractors, the ulnar nerve was located by releasing the brachial fascia just proximal to the cubital tunnel. Blunt dissection was carried out proximally using a curved mosquito hemostat to create a cavity between the subcutaneous tissue and the brachial fascia. A Cobb elevator was then gently introduced into this cavity to extend it at least 8 cm proximal to the medial epicondyle. A long nasal speculum was introduced into the cavity, and the brachial fascia and arcade of Struthers were released under direct visualization (Fig. 1). After removing the nasal speculum, Osborne's ligament was released. A distal cavity was then created between the subcutaneous tissue and Osborne's fascia, followed by the release of Osborne's fascia and the deep flexor-pronator aponeurosis. A short nasal speculum was introduced at this time to assist with clear visualization of the structures (Fig. 2). After complete release of all potential sources of structural nerve compression, the stability of the ulnar nerve was tested by moving the elbow through the full range of motion. If the nerve remained within the cubital tunnel throughout elbow flexion, it was considered stable.
If the nerve displaced onto the medial epicondyle during flexion or if it did not sit well within the cubital tunnel, it was considered unstable. In cases where instability was identified intra-operatively, the skin incision was extended by 1 cm proximally and distally to transpose the nerve anteriorly. The nerve was then carefully lifted from its bed with its accompanying longitudinal vascular supply intact. Segmental feeding vessels were identified and ligated to prevent tethering. Neurolysis of the posterior motor branches from the main ulnar nerve was performed to allow adequate anterior transposition if there was tension. The medial intermuscular septum was also excised as part of the anterior transposition. A fascial sling raised from the underlying muscle fascia was created to prevention slippage of the nerve after transposition (Fig. 3). After skin closure, a soft dressing and an elastic bandage were applied. Early flexion and extension of the elbow, though not supination or pronation, were encouraged. Thirty patients underwent simple decompression of the ulnar nerve, and the other 11 underwent anterior transposition of the ulnar nerve.
Statistical analysis
SPSS Statistics version 18.0 (SPSS Inc., IBM®, Chicago, IL, USA) was used for statistical analyses. Grip strength, pinch strength, two-point discrimination, and DASH score before surgery were compared to values at postoperative 2 years using paired t-tests. Nine independent variables were examined to identify the determinants of the clinical outcome assessed via DASH score at postoperative 2 years: age, sex, duration of symptoms, preoperative measures (grip strength, pinch strength, two-point discrimination, motor nerve conduction velocity, and Dellon grade), and surgical technique (simple decompression or anterior transposition). The Pearson correlation coefficient and the Spearman rho correlation coefficient (r) were used to evaluate the associations for continuous or non-parametric variables, respectively. The level of significance was set at p<0.05.
RESULTS
No postoperative complications occurred. At postoperative 2 years, grip strength increased from a mean of 19±10 kg to 31±11 kg (p<0.001), and pinch strength increased from a mean of 3.2±1.7 kg to 4.1±2.0 kg (p=0.008). The mean two-point discrimination improved from 6.0±2.5 mm to 3.2±1.2 mm (p<0.001). The mean DASH score improved from 31±24 to 15±15 (p<0.001) (Table 2). According to the modified Bishop Scale, excellent results were observed in 34 patients, good results in six, and fair results in one. The patient with fair results, who had in situ decompression as an index procedure, underwent anterior subcutaneous transposition of the nerve at 15 months postoperatively and reported improved symptoms after revisional surgery.
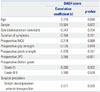
Linear regression analysis of DASH scores at postoperative 2 years indicated correlations in age (r=0.316, p=0.016), preoperative grip strength (r=-0.576, p=0.019), and two-point discrimination (r=3.066, p<0.001) (Table 3). There were no correlations observed between either of these outcome measures and the surgical procedure (simple decompression or anterior transposition of the ulnar nerve) according to the stability of the ulnar nerve.
DISCUSSION
In this study, we have shown that simple decompression and anterior subcutaneous transposition of the ulnar nerve based on preoperative and intra-operative assessment of ulnar nerve stability are safe and effective strategies for treating cubital tunnel syndrome. In a prospectively followed cohort of 41 patients treated with this tailored approach, grip and pinch strength were significantly increased, and two-point discrimination was significantly improved at postoperative 2 years. According to the modified Bishop Scale, 34 patients had outcomes rated as excellent, six as good, and one as fair. Significant correlations were observed between a worse DASH score at postoperative 2 years and older age, worse preoperative grip strength, and worse preoperative two-point discrimination.
According to a survey study, anterior transposition of the ulnar nerve is the most commonly performed procedure for operative treatment of cubital tunnel syndrome.12 A human cadaveric study showed that traction on the ulnar nerve during flexion of the elbow is a major cause of increased intraneural pressure and argued that only an anterior transposition procedure could effectively relieve the symptoms caused by neural traction.14 However, transposition of the ulnar nerve requires extensive dissection and puts the vascularity of the nerve at risk. In addition, a cost-benefit analysis has shown that the total costs associated with transposition of the ulnar nerve are significantly higher than those associated with simple decompression. 23 Simple decompression of the ulnar nerve presents several advantages over anterior transposition, including preservation of the blood supply to the nerve and shorter operative and rehabilitation times.11524
A previously published review of nonrandomized studies by Bartels, et al.24 found that simple decompression of the ulnar nerve has the most favorable outcomes. However, this analysis may be prone to substantial selection bias due to its use of nonrandomized data. In 2007, Zlowodzki, et al.15 conducted a meta-analysis of randomized, controlled trials comparing ulnar nerve transposition with simple decompression for the treatment of cubital tunnel syndrome in patients without a prior traumatic injury or surgery involving the affected elbow. They found no significant differences in postoperative motor nerve conduction velocities or clinical scores when comparing simple decompression with ulnar nerve transposition.15 However, two of the four trials included in this meta-analysis excluded patients with ulnar nerve subluxation, limiting the clinical applicability of the results of this study.
Most surgeons regard ulnar nerve subluxation or dislocation as an indication for ulnar nerve transposition. Bimmler and Meyer18 found that anterior transposition improves the clinical outcome for patients with ulnar nerve instability. Keith and Wollstein19 conducted simple decompression or anterior transposition according to the intra-operative stability of the ulnar nerve and found that 90% of their patients improved in terms of upper limb function. We also performed the tailored surgical approach based on the ulnar nerve stability test. This study showed that the tailored approach using either simple decompression or anterior transposition using a minimal incision, depending on the absence or presence of ulnar nerve instability, is safe and effective and is associated with an excellent clinical outcome in the majority of patients.
In 1981, Foster and Edshage25 reported that advanced age, prolonged duration of symptoms, and weakness of intrinsic muscles are the preoperative factors related to worse outcomes following operative treatment for cubital tunnel syndrome. However, the authors included not only idiopathic but also trauma-associated cubital tunnel syndrome and retrospectively assessed the clinical outcomes using an author-reported outcome measure. Our analysis showed that advanced age, weaker grip strength, and diminished two-point discrimination were correlated with worse outcomes as measured via DASH score at 2 years. Notably, this study did not find a correlation between the preoperative Dellon grade and worse clinical outcomes.
There were several limitations to this study. First, there was no control group of patients treated either non-operatively or with an alternative surgical procedure. Second, we used two outcome measures, the modified Bishop Scale and the DASH score, to estimate the clinical outcomes after surgical treatment; however, there is no reliable, reproducible, and valid outcome measure for cubital tunnel syndrome.26 An instrument reflecting patient-reported outcomes and satisfaction in combination with quantitative clinical findings is needed for standardized assessment of patients with cubital tunnel syndrome to accurately assess the clinical outcomes of surgical treatment for this common ulnar neuropathy. Third, this study included only a limited number of cases with a relatively short follow-up period.
In conclusion, we found that ulnar nerve stability-based surgery involving either simple decompression or anterior transposition for idiopathic cubital tunnel syndrome was a safe and effective strategy for surgical treatment following the failure of non-operative management, based on the results of our 2-year follow-up. Older age, worse preoperative grip strength, and worse two-point discrimination were associated with worse outcomes at 2 years. Future studies will investigate longer-term outcomes in a larger patient cohort.




 XML Download
XML Download