

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The rotational conflict in total knee arthroplasty (TKA) was mainly caused by the rotational mismatch of femur and tibia.1,2,3 Malpositioning and malorientation caused by the rotational conflict are the main causes of anterior knee pain and stiffness after surgery in a clinical aspect. And femoro-tibial subluxation and polyethylene (PE) wear give an impact even on the longevity of TKA.1,3,4,5,6 Even rotating flatform mobile bearing TKA, which helps to address such an issue, is still faced with difficulty in the subsurface wear. Studies on each rotation standard of femur and tibia actively been pursued so far. However, since the rotation of a knee joint includes factors coupled with both femur rotation and tibia rotation, it is better to realize rotational correlative relationship between the femoral and tibial components rather than to independently set rotational axis of each component in order to actually address the rotational conflict.7,8
The rotation of femur and tibia appears at the last extension of a joint knee in the form of screw home movement. It represents that tibia is relatively externally rotated for femur at the extension of a knee joint.7,9 Accordingly, the rotation angle of tibia for femur at the extension is determined by the rotation of femur and screw home movement. The rotation of femur varies depending on an operation, and screw home movement can happen differently in each knee. For such reasons, it is very difficult to synchronize the rotation of femur and the rotation of tibia during TKA operation.
Therefore, femoro-tibial axial synchronizer instrument, which helps to synchronize the rotation of femur and the rotation of tibia when screw home movement occurs, was designed to address the problem, and the prospective study was performed after TKA operation to identify through CT whether the rotation of femur and tibial components is matched.
MATERIALS AND METHODS
Study subjects
The prospective study had been performed from August 2009 to February 2010 on 66 patients (132 knees), who received bilateral TKA operation. Excluded were patients who had history of trauma to the pelvis or lower limb, a neuromuscular disorder, or prior surgery of the knee, hip, or pelvis, and more than 10 degrees of flexion contracture after operation. Consequently, 54 patients or 106 knees were analyzed. All patients received TKA using extramedullary (EM) alignment by a single surgeon (JGS), and two types of prosthesis-PCS (Scorpio posterior-cruciate-sacrificing PCS, Stryker, NJ, USA)- and NRG (Scorpio NRG, Stryker, NJ, USA)- were used for the operation. Patients were 68 years of age on average (range, 58-79), and patients received informed consent from this medical center and were approved by the Institutional Review Board of this medical center. Five days after the operation, their rotation axis was measured with the use of Transverse CT scans (X-Vigor, Toshiba Medical Inc., Tokyo, Japan), and clinical outcomes such as knee society score for 3 years after their operation and their radiologic outcomes with alignment precision were analyzed.
Femoro-tibial axial synchronizer (Linker)
Anteromedial limited parapatellar approach was used, and distal femoral block was set after soft tissue balancing. EM axis guider was used to check femur's coronal axis and sagittal mechanical axis, thereby determining femoral component's rotation. When transverse axis of distal femoral block nearly approached surgical transepicondylar axis (TEA), distal femoral resector was installed, and knee extension was made. This femoro-tibial axial synchronizer was designed to match the anteroposterior axis of femur and knee center, and is aimed at achieving femoro-tibial synchronization by using the inter-connected instrument of distal femoral resector and proximal tibial resector (Fig. 1).
After anterior condylar skim cut of femur, distal femoral resector was installed (Fig. 2). With the consideration of screw home movement, knee extension was made. After that, a connector with a plane such as proximal tibial resector was inserted into a slot of distal femoral resector, and axial synchronizer was installed (Fig. 3). The tail of proximal tibial resector presenting femur's coronal and sagittal axis was synchronized with tibia's coronal & sagittal axis (Fig. 4). AP pin was inserted for fixation by making it parallel with the AP plane of distal femoral resector. After that, proximal tibial resector was installed in the status of knee extension, and Linker was completed. After detachment of synchronizer, tibial resection was done, and tibial AP axis was then marked on the central part parallel with two AP pins. AP axis of tibial plate was synchronized with or parallel with the marked tibial AP axis (Fig. 5). After distal resection of femur, component was inserted. This utilizes the vertical relationship of the femur rotation and the tibia rotation with AP axis. When femeur's AP pin was parallel with tibia's AP pin, femoral component has a parallel relationship with a tibial component.
Operative procedures
Modified antero-medial parapatellar incision of Insall was used to make an approach. After soft tissue balancing, extramedullary technique was used to install distal femoral block. The connector to which proximal tibial resector was attached was inserted into distal femoral resector's slot, and EM axis guider was then used to adjust femur's coronal axis and sagittal alignment for synchronization. Then, a pin was inserted into proximal tibial resector. At this time, proximal tibial resector's AP pin was parallel with femoral resector's AP pin. After the removal of connector, the bone resection of proximal tibia and distal femur was performed, and a component was then inserted. As a result, femoral rotation matched with tibial rotation in the inter-related status, and planes were parallel even in coronal plane. Patella resurfacing was routinely performed, and implants became fixation with cement.
Evaluation of femoral and tibial rotation
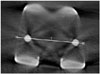
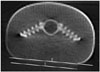
By performing postoperative CT scans, we measured the rotation of femoral and tibial component after operation. Transverse CT scans (X-Vigor, Toshiba Medical Inc., Tokyo, Japan) was used from tibial tuberosity to femoral distal metaphysic to take photos at 2.5 mm intervals. A patient's lower extremities were maximally extended in supine position, and photos were taken under the condition of non-internal or non-external rotation. Femoral component rotational axis was defined as a line linking the posterior margins of both pegs (Fig. 6), and tibial component was also defined as a line linking posterior margin of keels (Fig. 7). In doing so, the difference in the two component's rotation was analyzed. To evaluate inter-observer variability, three independent observers measured rotational axis of the femoral component and surgical TEA's angle.
Statistical analysis
Rotation's margin of error was set as about 5 degrees. This study was designed with more than 90% of statistical power and less than 5 degrees of error margin. The sample size of this study was more than 104 knees, and 106 registered knees were investigated further for precise evaluation. We examined the results of this study through one-sample proportions test, and utilized two-way random effects model of interclass correlation coefficients (ICC) to analyze statistical significance of inter-observer difference.
RESULTS
Comparative analysis of femoral component's rotational axis and tibial component's rotational axis showed that tibial component was internally rotated for femoral component at an average angle of 0.8°, and that all inter-observer repeated observations had no statistical significance at ±2.1°. The ICC about inter-observer variability was 0.96 indicating excellent agreement.
Femoral component was externally rotated for surgical TEA at an angle of 1.6° (range: from 4.8° of internal rotation to 7.9° of external rotation, SD=2.2°). In case of 97 out of 106 knees (91.5%). femoral component was rotated for surgical TEA at an angle of less than 5°. Tibial component was externally rotated for surgical TEA at an average angle of 0.9°, and outliers with more than 5 degrees were 6 knees, and variance was SD=3.1° (Table 1).
Mean alignment of the femoral component in the coronal plane was 89.5±2.5° (83.4-97.2°) postop and mean alignment of the tibial component was 90.3±2.1° (85.3-94.1°) postop. And the average tibial component posterior inclination was 4.8±2.1 (1.9-8.1) degrees.
Regarding ROM of postoperative 3 years, averages were 124.3±12.4 degrees, postoperative KSS score was 92.7±7.0 (62-100). There was no implant-related revision during 3 years.
DISCUSSION
Component's rotation in TKA is very important, and malrotation gives an impact on flexion instability, tibiofemoral and patellofemoral kinematic problem, and clinical outcome.1,10,11 In this respect, rotation alignment of femoral component and tibial component is significant, and the correlation of the two component's rotation is also important. Until now, there have been many studies on the rotation alignment, however, no absolute standards have yet been made.12,13,14
As a standard of femoral component's rotational axis, there are many methods, such as posterior condylar axis, Whiteside anteroposterior axis, transepicondylar axis, and flexion gap rectangularity balancing, but each method has an issue of variation.8,15 Among various methods, the method of making rotation with the focus of TEA has been known to have the least individual variation.2,6,11,16,17 Since TEA is the approximate value of flexion-extension axis and the origin of both collateral ligaments, it is considered as the most valid reference in many studies.4,7,8,18 As a standard of tibial component's rotation, medial one-third of tibial tuberosity proposed by Insall has most widely been used. However, since it is independent from femur's transepicondylar axis, rotational axis of femur and tibia should be set respectively. As described by Akagi, et al.,19,20 tibial component is extremely inclined to make external rotation compared with new anteroposterior axis perpendicular to femur's transepicondylar axis, and is likely to have no rotational correlation with femur component. Self-alignment of a conforming mobile tibial insert method using floating insert was proposed.16 The method has an advantage of femoral component's rotation and insert, and also correlated with tibial component rotation. However, according to Ikeuchi, et al.,10 self alignment method has a problem which makes tibial component to have more internal rotation.2 In spite of component's rotational axis and the importance of its orientation, standards related to the issue are not clear. Even though there is no problem in each rotation, rotation axis of each component can be different, which may lead to some problems.
Moreover, it is screw home movement that should additionally be taken into account. The screw home movement is the phenomenon where external rotation of tibia for femur occurs in normal knees at the extension of a knee joint, and it is seen as complex function of surface geometry, tension of ligaments and muscle.7,9 Regarding the motion in TKA, some studies found that the screw home movement did not occur, but the study conducted by Ishii, et al.9 revealed that muscle's activity significantly influenced screw home mechanism, more than ligaments did. If screw home movement occurs in knees after TKA operation, rotational congruency should be confirmed at the full extension of knees, and then femur and tibia's rotational matching should be performed.
In fact, there are many other techniques in dealing with rotational coupling. In case of measured resection technique, femur bone and tibia bone are independently resected with uncertain standards. In case of gap technique, tibia rotation is fixed at medial 1/3 of tuberosity, bone resection is made, and then rotation is decided.5,13,14,16,17 In addition, there are many difficulties in determining standards about screw home movement's variability and femoral external rotation. Because of difficulties, it is not easy to synchronize femoral component's rotation and tibial component's rotation, and it is necessary to determine the rotational axis of the two components with one absolute standard. As a solution of rotational conflict, the femur and tibial rotational synchronization can reduce polyethylene wear, prevent stiffness and patellofemoral maltracking, thereby weakening anterior knee pain. Furthermore, it possibly answers the long-debated question about fixed bearing and rotating platform bearing.
Ideal gap space should be perpendicular to the mechanical axis and matched to the component size. Furthermore, gap space between femur and tibia should be parallel and femoral resectional plane should be correlated to the femoral surgical TEA. Linker is a connecting instrument of femur and tibia. If it is used for bone resection, the femoral component has a parallel relationship with the tibial component in coronal plane, and coronal and rotational axes are matched to keep extension gap's rectangularity. Therefore, ideal gap space can be made by using Linker. In addition, AP axes are synchronized at full extension before resection of lateral femoral condyle and knee extension is made at the time of installation of distal femoral block and proximal tibial resector to receive rotational alignment with consideration of screw home mechanism.
There were some limitations in the present study. First, it is difficult to evaluate the rotational alignment because scanning direction of CT scan and flexion contracture easily affect the accuracy of measurement. In addition, the interval (2.5 mm) was slightly large with which peg holes and posterior margin may not clearly be detected. Second, there were nocomparative group (without Linker). Third, we chose the size of tibial plate not to be overhanged, nevertheless, rotational alignment could easily be changed if surgeons emphasized the coverage. Even though the use of a Linker can't be an absolute standard of rotational alignment, rotational conflict is likely to be minimized by synchronizing femur rotation with tibial rotation.
In conclusion, to address the rotational conflict of femur and tibia, femoro-tibial synchronizer (Linker) helped to improve the orientation and positioning of both the femoral component and the tibial component, and to increase the correlation of the rotational axis of the two components.






 XML Download
XML Download