

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Neointimal coverage over stent struts emerged as an important clinical issue after it was reported that incomplete strut coverage might be associated with the occurrence of late stent thrombosis following drug-eluting stent (DES) implantation.1,2,3,4 Optical coherence tomography (OCT) is a useful tool that has excellent resolution for confirming neointimal stent strut coverage.5,6 Although several variables such as the implantation of sirolimus-eluting stents (SESs)7,8 and acute coronary syndrome9,10 were reported as risk factors for delayed strut coverage in previous OCT studies, the relationship of specific medications (i.e., statins) with strut coverage is not fully understood. Statins are the most widely used lipid-lowering agents in patients with coronary artery disease. These drugs reduce inflammation and enhance endothelial function via pleiotropic effects.11 Previous in vitro and animal studies reported that statins regulate the migration and proliferation of smooth muscle cells and control neointimal formation.12,13,14,15 However, there are no human data that assess the impact of statin treatment on strut coverage after DES implantation. Therefore, we conducted a randomized OCT study to evaluate the effect of statin treatment on DES strut coverage.
MATERIALS AND METHODS
Study design and patient enrollment
The present study consisted of subgroup analysis of a previous randomized OCT study16 and evaluated the impact of statin treatment on strut coverage. The previous OCT study was performed to compare strut coverage 6 months after Nobori biolimus-eluting stent (N-BES, Nobori®, Terumo Corporation, Tokyo, Japan; n=60) or SES (Cypher™, Cordis Corp., Miami Lakes, FL, USA; n=60) implantation. The inclusion and exclusion criteria of the OCT study were provided in the previous report.16 Written informed consent was obtained from all participants, and the Institutional Review Boards of our institute approved this study. In total, 60 patients were enrolled in this study and randomly treated with pitavastatin 2 mg or pravastatin 20 mg, beginning on the day of stent implantation. Stenting (SES or N-BES) was also randomly allocated. Thus, four groups were created as follows: pitavastatin-N-BES group (12 patients), pitavastatin-SES group (17 patients), pravastatin-N-BES group (18 patients), and pravastatin-SES group (13 patients). Post-intervention OCT examinations were performed for all patients immediately after DES implantation. Among 60 patients, 6-month follow-up angiography was not performed for three patients, the OCT catheter could not be passed through the lesion due to severe angulation in three patients, and there was poor image quality in two patients. Therefore, follow-up OCT evaluation was performed for 52 patients as follows: pitavastatin-N-BES group (10 patients), pitavastatin-SES group (15 patients), pravastatin-N-BES group (14 patients), and pravastatin-SES group (13 patients) (Fig. 1). Blood samples to evaluate lipid profiles were obtained at the time of stent implantation and follow-up angiography. All patients were clinically followed up 1, 3, and 6 months after stent implantation.
Coronary intervention and quantitative coronary angiography analysis
All patients received at least 75 mg of aspirin and a loading dose of 300 mg of clopidogrel at least 12 h pre-intervention. Unfractionated heparin was administered to maintain the activated clotting time at >250 s. All percutaneous coronary interventions were performed according to current standard techniques. Post-intervention, dual antiplatelet therapy with aspirin 100 mg and clopidogrel 75 mg daily was prescribed for 12 months.
Quantitative coronary angiographic analysis was performed before and after stent implantation as well as at follow-up, using an offline quantitative coronary angiographic system (CASS system, Pie Medical Instruments, Maastricht, the Netherlands) in an independent core laboratory (Cardiovascular Research Center, Seoul, Korea). Using the guiding catheter for magnification and calibration, reference vessel diameters and the minimal luminal diameter were measured from diastolic frames in a single, matched view showing the smallest minimal luminal diameter. Late loss was defined as the difference between the post-procedure and follow-up minimal luminal diameters.
OCT imaging and cross-sectional analysis
Immediately and 6 months after the intervention, OCT of the target lesion was performed using a frequency-domain OCT system (C7-XR OCT imaging system, LightLab Imaging, Inc., St. Jude Medical, St. Paul, MN, USA). For this study, OCT cross-sectional images were generated at a rotational speed of 100 frames per second while the fiber was withdrawn at a speed of 20 mm/s within the stationary imaging sheath. All OCT images were analyzed at a core laboratory (Cardiovascular Research Center, Seoul, Korea) by analysts who were blinded to patient and procedural information.
Cross-sectional OCT images were analyzed at 0.2-mm longitudinal intervals. Stent and luminal cross-sectional areas (CSAs) were measured, and the neointimal hyperplasia (NIH) CSA was calculated as the stent area minus the luminal CSA. NIH thickness was measured as the distance between the endoluminal surface of the neointima and the strut.8 An uncovered strut was categorized as an NIH thickness=0 µm.8 A malapposed strut was defined as a strut that had detached from the vessel wall by ≥130 µm (N-BES) or ≥160 µm (SES).17,18 The percentage of uncovered or malapposed struts was calculated as the ratio of uncovered or malapposed struts to total struts in all OCT cross-sections. Intrastent thrombi were defined as irregular masses protruding into the lumen by more than 250 µm at the thickest point.19
Statistical analysis
Statistical analysis was performed using Statistical Analysis System software (v. 9.1.3., SAS Institute, Cary, NC, USA) and R version 2.15.1 (R Development Core Team, Vienna, Austria, http://www.R-project.org). Categorical data were presented as numbers (%) and compared using the chi-square or Fisher's exact test. Continuous data were presented as the mean±SD and compared using a paired t-test, Student's t-test, or the Mann-Whitney U test. To avoid problems of sample size inflation and correlated data, only patients with one target lesion were included in the study. Cross-section analysis or strut-level analysis may not be straightforward due to the congregation of struts within each lesion in an interindividual manner. For this analysis, we performed multilevel regression model analysis. Specifically, the patient and lesion data were incorporated as random effect components using the lme4 package with R (http://cran.r-project.org/web/packages/lme4/index.html).20 Pearson's correlation analysis was performed to evaluate the relationship between low-density lipoprotein (LDL) cholesterol levels and the percentage of uncovered struts. Values of p<0.05 denoted statistical significance.
RESULTS
Baseline clinical and angiographic characteristics were similar between the pitavastatin-treated groups and pravastatin-treated groups (Table 1). Significant reductions of LDL cholesterol levels were observed at the 6-month follow-up time point (reduction: 24 mg/dL in the pitavastatin-treated group, p<0.001; 21 mg/dL in the pravastatin-treated group, p= 0.003). Follow-up LDL cholesterols level less than 70 mg/dL were achieved in 10 patients (34.5%) in the pitavastatin-treated group and 5 patients (16.1%) in the pravastatin-treated group (p=0.101). OCT findings were also similar between pitavastatin-treated patients and pravastatin-treated patients (Table 2). The percentages of uncovered struts at the 6-month follow-up OCT were 19.4±14.7% in pitavastain-treated patients (n=25) and 19.1±15.2% in pravastain-treated patients (n=27) (p=0.927); conversely, the values were 23.3±16.6% in SES-implanted patients (n=28) and 14.5±10.9% in BES-implanted patients (n=24) (p=0.026).
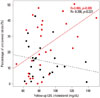
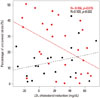
In all of 52 patients, follow-up cholesterol levels of less than 70 mg/dL were associated with smaller percentages of uncovered struts (less than 70 mg/dL vs. 70 mg/dL or more; 12.5±12.2% vs. 21.5±15.1%; p=0.058). Although the percentage of uncovered struts among SES-implanted patients was significantly lower in patients with follow-up LDL cholesterol levels of less than 70 mg/dL (less than 70 mg/dL vs. 70 mg/dL or more; 10.1±12.4% vs. 26.9±15.6%, respectively; p=0.025), there were no significant differences in the percentage of uncovered struts among BES-implanted patients between those with follow-up LDL cholesterol levels of less than 70 mg/dL (14.6±12.7%) and those with levels exceeding 70 mg/dL (14.4±10.5%; p=0.971). Fig. 2 presents the relationship of follow-up LDL cholesterol levels with strut coverage according to DES type. The percentage of uncovered struts was significantly correlated with follow-up LDL cholesterol levels (r=0.486; p=0.009) in SES-implanted patients but not in BES-implanted patients. Fig. 3 presents the relationship of the degree of LDL cholesterol reduction with strut coverage according to DES type. The percentage of uncovered struts was also significantly correlated with the degree of LDL cholesterol reduction (r=-0.456; p=0.015) in SES-implanted patients but not in BES-implanted patients.
DISCUSSION
Previous studies identified several factors that were associated with delayed strut coverage, such as SES implantation,7,8 acute coronary syndrome,9,10 the time interval between DES implantation and follow-up OCT,21 baseline high-sensitivity C-reactive protein levels,22 the stent diameter,23 diabetes mellitus,23 and American Heart Association/American College of Cardiology type B2/C lesions.23 Although several studies revealed that statins have beneficial effects on both mature endothelial cells and endothelial progenitor cells,24,25,26,27 there are no human data associating the use of statins with an acceleration of strut coverage after DES implantation. Wang, et al.14 demonstrated that atorvastatin pretreatment could accelerate both neointimal coverage and reendothelialization after SES implantation in a minipig model. Another animal study using a wire-mediated vascular injury model in mice reported that fluvastatin has protective effects against impaired reendothelialization in sirolimus-treated arteries.24 The mechanism by which statins protect against delayed vascular healing is linked to their ability to modulate smooth muscle cell proliferation and migration and increase circulating endothelial progenitor cell counts.14,24 Experimental animal studies reported that each statin has different effects according to its water solubility.28,29
In this study, strut coverage was compared between pita-vastatin-treated lesions and pravastatin-treated lesions, and we hypothesized that different statins may differentially affect OCT-based strut coverage in DES-implanted lesions. Compared to pravastatin (a hydrophilic statin), pitavastatin (a fully synthetic lipophilic statin) has powerful efficacy comparable with that of atorvastatin and rosuvastatin.30,31 In the present study, a significant difference in strut coverage was not observed between the pitavastatin-treated groups and pravastatin-treated groups; however, greater DES strut coverage was significantly related with lower follow-up LDL cholesterol levels and greater reductions of LDL cholesterol levels in SES-implanted lesions, but not in BES-implanted lesions.
These findings suggest that reducing LDL cholesterol levels alone has a role in strut coverage after first-generation DES implantation. However, as mentioned previously, the primary mechanism by which statins modify the vascular healing process is considered to involve a pleotropic effect rather than a direct LDL cholesterol-lowering effect. Therefore, this discrepancy might be explained by the fact that a lower LDL cholesterol level is one indicator of the intensity of the pleotropic effect of statins in the vascular healing process. Additionally, the relationship between follow-up LDL cholesterol levels and strut coverage was not observed for next-generation DESs (i.e., BESs). A possible explanation for this finding is that the vascular healing response to statins or lower LDL cholesterol levels could be different according to the type of DES. Compared to SESs, BESs have several different characteristics, including a bioresorbable polymer carrier (poly-lactic acid), as well as coating only on the abluminal stent surface to allow the direct release of lipophilic biolimus into the vessel wall.32,33 Differences in the polymer, drug, or drug-eluting period between BESs and SESs may influence the degree of strut coverage according to the LDL cholesterol-lowering effects of statins.
The present study has some limitations. First, although our study was designed as a randomized trial, the study population included a relatively small number of patients. We feel that a future study with a larger sample size would be needed to confirm our findings. However, our main findings could provide a clue, suggesting the possible relationship of lowering LDL cholesterol or use of statin with the vascular healing process. Second, all control groups received statin therapy. Therefore, we could not evaluate the effect of statin therapy on strut coverage by making comparisons with patients who did not receive statin treatment. However, a control group with no statin treatment would not be ethically justified in current clinical practice for DES-implanted patients with coronary artery disease.
In conclusion, this randomized study revealed a protective effect of statins against delayed strut coverage in SES-implanted patients who achieved lower follow-up LDL cholesterol levels (especially less than 70 mg/dL). This vascular healing effect of lower LDL cholesterol levels induced by statins could be different according to the type of DES implanted.



 XML Download
XML Download