

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
IgG4-related sclerosing disease is a systemic disease characterized by extensive IgG4-positive plasma cells and T-lymphocyte infiltration of various organs. Hamano, et al.1 reported that patients with sclerosing pancreatitis had a high serum IgG4 concentration with abundant and diffuse infiltration of IgG4-positive plasma cells in the pancreas. Since that original report, abundant IgG4-positive plasma cell infiltrates have been demonstrated in many extrapancreatic sclerotic lesions.2 Involvement of the heart in IgG4-related sclerosing disease is rare.3 The clinical presentation depends on the involved tissues; however, the histopathologic findings seem to be similar regardless of location.4 We report a case of IgG4-related sclerosing disease involving cardiac conduction system, that induced recurrent syncope in a middle aged female patient.
CASE REPORT
A 55-year-old woman was admitted to our institution with recurrent episodes of syncope and dizziness. She had no underlying disease, including autoimmune diseases. The patient's past medical history was not significant for any medications or illicit drugs. The electrocardiogram on admission showed first-degree atrioventricular block with a prolonged PR interval of 240 ms (Fig. 1A). Furthermore, the patient demonstrated atrial fibrillation (Fig. 1B) and a sinus pause of six seconds during an exercise test (Fig. 1C). During ambulatory Holter monitoring, frequent episodes of sinus pauses and atrial fibrillation were observed.
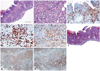
Transthoracic echocardiography and magnetic resonance imaging demonstrated a mass extending from the superior venacava (SVC)-right atrium (RA) junction to the right atrium posterior wall and interatrial septum (Fig. 2Aa). Fluorodeoxyglucose positron emission tomography showed increased uptake in a mass involving the RA wall and interatrial septum (Fig. 2Ab). No other evidence of abnormal uptake was noted. Transcutaneous cardiac biopsy was performed, however, failed to obtain enough tissue to confirm the histologic diagnosis. Therefore, the patient underwent open chest biopsy. Histologically, the lesion was composed of proliferating IgG4-positive plasma cells and lymphocytes (Fig. 3). The ratio of IgG4/IgG positive cells was 68% in average. And absolute number of IgG4-positive cells was approximate 146.5 per high-power field in the hottest area. These findings are consistent with IgG4-related sclerosing disease.2
The cardiac mass involved the SVC and interatrial septum, and was inoperable. Additional chemotherapy or steroid therapy was not performed because of patient's preference. A permanent VVI-type pacemaker was implanted due to frequent sinus pauses and syncope. During a one-year follow-up, the patient had no additional episodes of syncope, and the mass showed no evidence of progression (Fig 2Ac and B).
DISCUSSION
IgG4-related sclerosing disease is a relatively newly found entity with distinct clinicopathologic characteristics. The disease was originally discovered in patients with autoimmune pancreatitis and an elevated serum level of IgG4. It is characterized by extensive IgG4-positive plasma cells and T lymphocyte infiltration of various organs. Cardiac involvement of this disease is extremely rare. Recent reports described cardiovascular IgG4-related sclerosing disease as pericarditis and periarteritis related to heart failure or angina.5-7 However, to our knowledge, involvement of the cardiac conduction system has not been reported.
The cause and clinical progress of IgG4-related sclerosing disease remain undefined. Some studies report a rapidly fatal outcome of this disease.8 As the cause is unknown, there is no consensus on the optimal treatment approach. IgG4-related sclerosing disease has previously been suggested to be managed by corticosteroid and/or immunosuppressive therapies.9-11 In this case, we did not perform chemotherapy or corticosteroid therapy because of patient refusal. Instead, the patient's symptoms were managed by pacemaker implantation. Interestingly, tumor progression was not observed during a one-year follow-up period. Although the follow-up duration was short, we suggest that symptomatic management alone might be a possible option for treatment of this disease.
In summary, there has been no case in the literature of intracardiac IgG4-related sclerosing disease that involves the sinus and atrioventricular nodes. Our report suggests that IgG4-related sclerosing disease has a favorable prognosis and withhold steroid therapy. If there is no deterioration of symptoms, symptomatic management and regular follow-up might be a reasonable treatment option.


 XML Download
XML Download