

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The increased use of interventional procedures and laparoscopic cholecystectomy in the management of hepatobiliary disorders is associated with an increased incidence of hemobilia and HAA.1-3 HAA accounts for nearly 10% of hemobilia cases.4 Hemobilia and HAA have been associated with percutaneously placed stents5-7 and HAA with endoscopically placed expandable metal stents.8,9 A single case has been reported of massive hemobilia due to HAA after the extraction of a plastic biliary endoprosthesis.10 Here we report a case of hepatic artery pseudoaneurysm associated with a plastic biliary stent. Multiple factors were involved in the formation of the HAA and it was successfully managed by embolization.
CASE REPORT
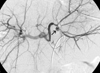
A 62-year-old woman was admitted to the hospital with fever and jaundice. She had been diagnosed with Klatskin tumor, Bismuth type IIIa. Two months before admission, percutaneous transhepatic biliary drainage catheters were inserted to segment 5 and 6 of the liver, and a plastic biliary stent (pigtail type, 10Fr, 10cm) was inserted into the left hepatic bile duct. One month before admission she underwent concurrent chemoradiotherapy. Computerized tomography shortly after chemoradiotherapy showed no dilatation of intrahepatic bile duct. On admission, the physical examination revealed jaundice and fever. Computerized tomography at admission showed multiple abscesses in both lobes of the liver and intrahepatic bile duct dilatation, but the percutaneous biliary drainage catheter and plastic biliary stent were well positioned (Fig. 1). Laboratory evaluation showed an elevation in total bilirubin to 11.2mg/dL and in white blood cell count to 18360/µL. The level of hemoglobin was 10.4g/dL, and the hematocrit was 31.4%. Two days after admission hematemesis occurred. Hemoglobin levels dropped to 7.7g/dL and hematocrit to 23.0%. Endoscopic evaluation showed hemobilia and migration of the biliary stent. Hepatic angiography revealed a pseudoaneurysm of 2cm in size at the proximal portion of segment 3 branch of the left hepatic artery where the tip of the plastic biliary stent was originally positioned prior to migration (Fig. 2). Two tornado coils, 4mm and 3mm (Cook, Denmark) were placed at the aneurysm. However, hematemesis occurred again four days after embolization, and a second angiography was performed, involving embolization with 1ml of a mixture of histoacryl 1ml and lipiodol 2ml. After the second embolization, cholestasis improved and no evidence of bleeding was noted. The patient was discharged 20 days later.
DISCUSSION
Many factors are associated with hemobilia, including aneurysm of the hepatic artery.4,11,12 In this case, we suspect that the stent was the cause of the aneurysm because the tip of the stent was at the site of the aneurysm. However, this may not be the only cause. Before the episode of hemobilia, we found multiple abscesses in the liver and elevated levels of bilirubin, suggesting increased intraductal pressure and cholangitis, and both could affect the formation of aneurysm.8 It has also been reported that radiation therapy increases the risk of stent-related complications.13 It therefore seems likely that the stent induced the aneurismal change of the hepatic artery in combination with radiation therapy, increased intrabiliary pressure, and cholangitis. Bleeding from the aneurysm started when the stent migrated, similar to the previously documented case where hemobilia occurred after the extraction of a plastic biliary stent.10
Since the mortality rate associated with rupture is 21%, aggressive treatment is recommended. Treatment modalities include embolization, reconstructive surgery, or ligation. For intrahepatic artery aneurysms, such as that presented here, embolization is the accepted treatment of choice.1,2
In summary, we report a case of hepatic artery pseudoaneurysm associated with a plastic biliary stent and successfully treated by embolization. The possibility of hepatic artery aneurysm should be suspected when hemobilia is associated with the migration of a biliary plastic stent.

 XML Download
XML Download