

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Various stabilization techniques have been evaluated for the management of spinal instability. Anterior fixation is generally used for anterior column disorders, or as an adjunct to posterior fixation for three-column injuries. However, several complications and limitations have been associated with this technique. Posterior fusion and fixation may be the optimal approach in patients who require multilevel decompression, particularly if the construct requires an extension to the upper cervical or thoracic spine, sometimes to the occiput. Additionally, the clinical and biomechanical results from numerous studies have shown that the combined anterior-posterior instrumentation and the posterior-only instrumentation models are significantly more rigid than the anterior-only model.1,2 Further, a previous study showed that there were no statistically significant differences between the combined anterior plate/posterior instrumentation model and the posterior instrumentation-only model.3 Overall, posterior stabilization is generally preferred for posterior and circumferential cervical injuries. Advancements in posterior cervical fixation have moved from a wiring procedure to hook and plate-screw systems, and more recently towards the versatile rod-screw system.
Since Roy-Camille et al.4,5 introduced posterior stabilization of the cervical spine with screws and plates, several reports have concluded that this system is biomechanically superior to posterior wiring, especially for extension and torsion.6,7 Clinical use of the plate and screw fixation systems is increasing and the results are encouraging.8-10 This technique, however, also has limitations. The predrilled holes in the posterior plates do not always line up evenly with the lateral masses, thus affecting the screw placement. Additionally, since the plates are difficult to contour because the position of the screw is constrained by the entry holes of the plate, screw back-out can occur, and the plate systems can not be easily adapted for extension to the occiput or thoracic spine. There is also a risk of implant failure and loss of alignment.11 More recently, a polyaxial screw and rod fixation system has been developed and is widely used to avoid these limitations. In this system, the screws can be placed first and the rod can be contoured in multiple planes. As a result, the screw-rod system is able to more effectively accommodate variations in size, spacing, and morphology of the lateral masses. In addition, this system is more easily extended to the occiput and across the cervico-thoracic junction. With this system, compressive or distractive forces can be applied. Recent studies have also reported that rod-screw fixations have better biomechanical stability than posterior plate fixations in vitro12,13 and a lower hardware-related complication rate.14
In this study, we review our clinical experience with the polyaxial screw-rod system, including the clinical and radiological outcomes of our 65 patients. In addition, we suggest detailed surgical techniques to reduce associated complications.
PATIENTS AND METHODS
Sixty-five consecutive patients who required posterior cervical and/or high thoracic stabilization using the Polyaxial Screw-rod System (Vertex; Medtronic Sofamor-Danek, Memphis, TN, Summit; Depuy Spine, Raynham, MA, USA) were operated on between July, 2003 and March, 2006. The patients included 44 men and 21 women (age range = 19 to 83 years; mean age = 53 years). The mean follow-up period was 8.8 months (range = 4 to 20 months).
The following factors were evaluated: morbidity level, disease entity, early postoperative CT scan to confirm satisfactory screw placement, dynamic plain X-rays for evaluation of fusion, segmental mobility, hardware integrity, and comparison of preoperative and postoperative spine stability. The adequacy of fusion was determined at approximately 4, 6 and 12 months postoperatively. Pseudoarthrosis was defined as a motion > 2.0mm between the laminae at the base of the spinous processes between the upper and lowermost fixed and fused levels on the flexion/extension plain radiographs.
Additionally, we evaluated the clinical outcomes as well as postoperative complications. Preoperative and final follow-up Visual Analog Scales (VAS) for neck and arm pain as well as Neck Disability Indices (NDI)15 were prospectively collected and used in this analysis. The American Spinal Injury Association Impairment Scale (ASIA)16 was used to classify the neurological status preoperatively and postoperatively. The measurement was assessed using a 10-point VAS with endpoint anchors of no pain (0 point) and severe pain (10 points). The NDI questionnaire is comprised of 10 single items related to activities of daily living. Each item has six predefined response categories, coded 0-5 on an ordinal scale. The scores reflected either the degree of neck pain or the degree of difficulty in performing certain actions due to neck pain. The lowest score (0) represented no problem or pain, whereas the highest score (5) represented maximum problems or pain. The pre- and postoperative arm and neck symptom VAS scores and NDI scores were compared using two-sample t tests paired for means. A p value of < 0.05 was regarded as significant
Surgical technique
The surgery was performed in a consistent fashion. Intubation was performed for cases with severe cervical stenosis or gross instability in an awake, fiberoptic fashion. The patient was then carefully turned to the prone position and the patient's head was placed in a Mayfield Cranial Fixation device with fluoroscopic guidance to assess the spinal alignment as well as to localize the pathology. The patient could then be prepped and draped in the standard fashion.
A standard midline incision was made that exposed all the levels to be fused. The lateral masses were exposed in a subperiosteal fashion to the lateral margins of the facet joints. If needed, reduction of the locked facets was performed with the use of a high-speed drill and a double-ended micro-elevator. Once the deformity was reduced, the lateral masses to be fused were decorticated with the drill. Great care was taken not to disturb the capsule at adjacent levels in order to prevent any iatrogenic instability.
Lateral mass screws were used at C1 and from C3 to C6, and pedicle screws were used at C2 and C7. Pedicle screws were also used if the construct was extended into the thoracic spine. Screw insertion was always performed prior to laminectomy or laminoplasty for posterior decompression of the spinal cord, except in laminectomy during intradural tumor surgery. In cases with tumors, screws can potentially interfere with detailed micro-work in tumor removal. Details and recommendations regarding screw insertion at each level and the selection of screws are included in the discussion section. Pilot holes were drilled in the appropriate lateral masses, and a manual drill was used to create a path for the screws. Fluoroscopy was used for C1 and C2 screw placement, whereas the sub- axial screws were generally placed using anatomic landmarks.
After screw placement, a decompressive laminectomy was performed. A rod was prepared to the appropriate length and contour of the patient so that it would easily pass through the heads of all polyaxial screws. Once the rod was positioned, it was secured to the heads of the screws using outer nuts. Before final tightening, each segment was distracted or compressed, as needed.
Bony fusion was performed by packing local autograft bone from the posterior elements into the facet joints and around the decorticated lateral masses, lateral to the rod. The morselized iliac crest bone is typically used if a long segment fusion is required. The procedure was easily adapted for occipitocervical or cervicothoracic fusions with the connection of suboccipital and thoracic stabilization, and was used in conjunction with combined anterior-posterior procedures or laminoplasty as needed. During the entire procedure, the retractors were intermittently released to avoid denervation of the erector spinae muscles. Routine closure was carried out and drains were left in place as needed.
RESULTS
A total of 486 screws were implanted in 65 separate patients. The lesions included 18 cases of tumors, 31 cases of degenerative disease including ossification of the posterior longitudinal ligament (OPLL), 14 cases of trauma and one case each of rheumatoid arthritis and Klippel-Feil Syndrome. Screw fixation was performed over an average of 2.9 spinal segments, with a range of one segment to six segments.
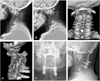
Decompressive laminectomies were performed in 58 patients. Posterior screw fixation combined with laminoplasty was carried out in 2 cases and combined with anterior decompression fusion in 5 cases. Occipitocervical fusion was performed in one Klippel-Feil Syndrome patient with myelopathy who showed occipitocervical and C1/2 instability with block vertebrae from C2 to C5 in preoperative studies. (Fig. 1) In this patient, cervical (C3, C4) lateral mass screw fixation was adapted for the occipitocervical fusion with the connection of the suboccipital plate (Summit Fixation System, DePuy AcroMed, Raynham, MA, USA). In two cases of long level cervicothoracic junctional area intramedullary tumors requiring long level laminectomies, screw fixation was performed solely in the cervicothoracic junctional area that had complicated biodynamic mechanisms.
In the evaluation of the early postoperative CT scans that were routinely performed in all patients, twelve (2.5%) screws had a suboptimal trajectory with no resulting vascular sequelae. Two out of these twelve screws were in one patient and resulted in postoperative right shoulder pain that required screw removal and reposition. (Fig. 2) After reoperation, the patient's symptoms subsided. Based on dynamic X-rays, no pseudoarthrosis was noted according to our criteria and no symptomatic adjacent segment angulations have been revealed to date. As for other complications, there was one case of dural tearing and two cases of screw-induced lateral mass fracture during surgery. We converted the screw trajectory to the modified Roy-Camille17 technique and used 4mm rescue screws in those cases. Other than the aforementioned, there were no screw pull-outs or hardware- induced complications. Additionally, there were no infections or other wound healing problems.
No patients had neurological deterioration (ASIA) after surgery. Concurrently, there were statistically significant improvements in the mean NDI and VAS scores from the preoperative evaluations to the late postoperative follow-up evaluations. Analysis of NDI scores showed preoperative scores averaging 38 ± 16.4 points, whereas at final follow-up, scores averaged 17 ± 14.9 points (p < 0.005). Regarding neck pain, the average preoperative VAS score was 8.15 ± 2.3, while at final follow-up it was 3.2 ± 3.0 (p < 0.001). The VAS score for arm pain preoperatively was 7.1 ± 2.3 compared with an average score of 2.3 ± 3.1 at the final follow-up (p < 0.001).
DISCUSSION
Lateral mass screw fixation
The cervical lateral mass screw and plate system has several advantages compared to wire/cable constructs. These include ease of application, lack of dependence on intact posterior elements, and immediate rigid fixation. Roy-Camille designed the first lateral mass screw plate system and published his extensive experience using these systems.4,5 Newer screw-rod systems can now extend rigid internal fixation from the occiput to the high thoracic spine as well as to the sub-axial cervical spine, with variable screw placement to accommodate the complex anatomy.
Several modifications on the Roy-Camille technique for lateral mass screw fixation have been proposed over the years.8,18,19 Roy-Camille et al.5 advocated using the mid-point of the articular mass as the starting point for screw placement in the subaxial cervical spine, and suggested that the surgeon drill perpendicular to the posterior plane of the spine and 10˚ laterally. The mid-point was determined by outlining the superior border at the cranial joint line, the inferior border at the caudal joint line, the lateral border of the lateral mass and the junction of the lamina and lateral mass forming the medial border.
Magerl's group recommended starting the drill hole 2-3mm medial and superior to the apex of the lateral mass and angling 30˚ upward and 25˚ outward. In a cadaveric study, An et al.18 sought to find the safest screw trajectory to prevent injury to the nerve root and vertebral artery. They found that the nerve root was at risk if the screws were placed with a marked cephalad direction. They recommended that the screws be inserted 30˚ laterally and 15˚ in the cephalad direction, starting 1mm medial to the center of the lateral mass from C3 to C6 in order to avoid injury to the nerve root and the vertebral artery. The currently accepted modification of this technique places the starting point 1mm medial to the mid-point and angles the drill 15-20˚ rostrally and 20-30˚ laterally .
The awl is used to mark the starting point and the drilling is started using a 2.3mm drill bit with a drill guide. The drilling commences in a vertical direction until the outer cortex is perforated. The drill is then introduced in the aforementioned direction. To reduce the possibility of slippage of the marking awl and guide drill, a small diameter diamond burr is helpful for perforation of the lateral mass cortex and for the initial guiding of the drill. The depth to be drilled and the appropriate length of screw were determined based on the measurements obtained on the patient's preoperative CT scans. The drill hole is tapped with a 3.5mm tap. To reduce the possibility of lateral mass fracture during subsequent screw fixation, drilling and tapping should be performed along the entire measuring length of each screw. Additionally, in order to insert the screw up to the measured length, a groove was set for each screw head at the medio-inferior side of the screw insertion point needing to be drilled. Although the screw system is polyaxial, slight inclination of the medial part of the lateral mass prevents the screw from advancing up to its entire length.
From C3 to C6, most of the screws placed in our series had a lateral mass screw length of 14mm. In a cadaveric study, the average vertical distance between the posterior midpoint of the lateral mass and the vertebral foramen from C3 to C6 was found to be approximately 9-12mm.20 Consequently, 14mm in an oblique direction should adequately span the lateral mass unicortically or bicortically. In accordance with this finding, Seybold et al.21 reported in a 1999 cadaveric study of unicortical and bilateral mass screw placement that there were no statistically significant differences in pull-out strength between unicortical and bicortical screws. Thus, we do not routinely attempt to use bicortical screws during lateral mass screw fixation in the subaxial cervical spine.
Although a lateral mass screw can be placed at C7 as described above, the lateral mass at C7 is somewhat elongated in a rostro-caudal direction and is thinner,22 so a pedicle screw may be more appropriate at C7. If a lateral mass screw is to be used at C7, great care must be taken so as not to insert too long a screw and injure the C8 nerve root. The use of short screws (12mm) and the use of more cephalad and lateral directions of screw trajectory can reduce the chance of nerve root injuries.23
Pedicle screw fixation
The description of transpedicle fixation in the cervical spine has been confined to the relatively large C2 and C7 pedicles. At C2, there is a significant risk of injury to the vertebral artery with a laterally directed lateral mass screw. At C7, the lateral mass is small, and a lateral mass screw could cause a C8 radiculopathy. Heller et al.24 found decreased pull-out strength for lateral mass screws inserted at both of these levels. Therefore, for anatomic and biomechanical reasons, pedicle screws are preferred at C2 and perhaps at C7.
For pedicle fixation at the C2 pedicle, the inferior facet of C1 was exposed. The medial and superior surfaces of the pedicle were identified. Based on cadaveric studies of Ebraheim et al.25 and Abumi et al,26 we routinely made the entry point at the transverse extension line of the midsuperior margin of the C2 lamina and 6-7 mm lateral to the lateral border of the spinal canal. The direction of the drill was about 25-30˚ medial to the sagittal plane and slightly cephalad or parallel to the C2-3 disc space under fluoroscopic guidance. Placement was also guided by direct visualization and palpation of the medial and superior aspect of the C2 pedicle. Drilling and tapping was performed without skiving using a lateral mass screw fixation technique. To reduce vertebral artery injury and to determine the appropriate screw diameter and length, we routinely performed preoperative 3D angiographic CT scans. In the rare cases of vertebral artery variations (including a high riding vertebral artery), adjustments in the entry point and/or direction of drilling and the screw diameter may be needed.
The fixation of C7 and upper thoracic (T1 to T4) pedicle screws were more complicated because of their small pedicle sizes and high risk of injury to major neurovascular structures. Furthermore, intraoperative lateral radiographic images are obscured by the shoulder girdles. The entry point selected for C7 screw placement was just lateral to the midline of the articular mass and just below the lower margin of the superior articular surface. A lamino-foraminotomy was performed at the levels that were to undergo instrumentation. The medial and superior surfaces of the pedicle were palpated and protected, and a 2.3mm drill bit was utilized to drill into the pedicle. According to morphometric studies of the C7 pedicle,18,27 the mediolateral and superoinferior outer pedicle diameters were 6.9mm and 7.5mm, respectively. The average mediolateral inner diameter was 5.18 mm and the medial angulation averaged 34˚. Considering these measurements, 3.5mm to 4.0 mm diameter screws were feasible. In our cases, we routinely used 3.5mm diameter screws. Based on measurements from preoperative CT images, 20 to 24mm length screws were placed parallel to the upper end plate in the sagittal plane, and ranged from 25˚ to 35˚ in the transverse plane relative to the midline.
For the high thoracic area, several screw insertion methods have been suggested.28-30 One method involves a more lateral entry point (i.e. the Weinstein approach30) with more convergence and a higher insertion angle, and the other involves a rather medial entry point (i.e. the Roy-Camille approach29) with less convergence and a smaller insertion angle. In the original technique described by Roy-Camille,29 the entrance point for screw insertion was situated in the intersection between a vertical line passing through the middle of the inferior facet and a transverse line passing through the middle of the transverse process. The screw was placed perpendicular to the posterior plane of the vertebrae and straight in a forward direction. Although screw placement with a straight, forward direction as used in the original Roy-Camille method may be safe in the lower thoracic levels, this technique has a higher incidence of penetration of the lateral wall of the pedicle in the middle and upper thoracic areas due to the medial inclination of the pedicle.31 Therefore, we routinely chose an entry point at the level of the superior border of the transverse process and 3mm lateral to the middle of the inferior facet, and drilling was directed to about 25˚ for T1, 20˚ for T2 anteromedially and 10˚ to 20˚ caudally. Before the tapping procedure, penetration of the pedicle cortical walls and the vertebral body anterior cortex should be confirmed with a 2mm-blunt tipped, slightly curved probe.
After screw fixation, the rods were connected with the desired kyphotic angulation. Abumi et al.26 recommended outer nut fixation from the caudal to rostral direction in order to preserve the kyphotic angle, but this method sometimes made it difficult to fix the lower nuts with the rods. To remedy this, we put the rod on the screw head and captured it with the nuts simultaneously, then tightened it from the caudal to rostral direction.
Fusion
As was previously mentioned, bony fusion was performed in all of our cases. It was performed with a morselized posterior element bone with or without the iliac bone into the facet joints and around the decorticated lateral masses, lateral to the rods. Although only short-term follow-ups have been performed in this group of patients, a six-month follow-up of the first 24 patients and a four-month follow-up of eight later patients did not reveal segmental motion in dynamic films with progressive bony fusion. We could not describe the exact fusion rate in our study group. CT scans showed bone fusion in the first 24 patients. (Fig. 3) In a recent study, Katonis et al.32 noted a fusion failure rate of 57% in patients treated with facet joint decortication and scraping without application of bone graft after the application of the lateral mass plate system. In contrast, they reported a 98% fusion rate in patients with bone grafts into the involved facet and under the plates. Therefore, additional bone grafts with the posterior polyaxial screw and rod fixation system seems to be the recommended procedure.
Complications
Several authors have reported cases treated with posterior screws with a plate or rod system.22,32,33 According to these reports, outcomes in terms of fusion rate, clinical symptoms, and stabilization were excellent and had low complication rates. Fusion rates have ranged from 91-100% with a less than 5% complication rate. The most considerable complications were induced by screws, and included neural or vascular injury due to screw malposition, facet violation and hardware loosening with screw breakage or screw pull-out. In 1996, Graham et al.33 reported that 6% (10/164) of screws were malpositioned, and three (1.8%) of those screws induced radiculopathy. Recently, Sekhon reported the results of lateral mass screw fixation with 1,026 screws in 143 patients. He reported that only 20 screws (1.9%) breached the transverse foramen and no patients complained of radiculopathy or vascular injury.23 In his series, 14 × 3.5mm screws were used in most cases of C3 to C6 lateral mass screw fixation, similar to our series, and the medial, superior screw angles were also the same as those used in our series. As previously mentioned, a detailed knowledge of the anatomy of this area with critical screw selection and trajectory is required to reduce screw-induced complications.
For C7 and upper thoracic pedicle screw fixation, the use of lamino-foraminotomy, which enables the surgeon to palpate and protect the medial and superior surfaces of the pedicle, may be the easiest and safest way to reduce the incidence of complications.
Reported implant failure is rare. In a large series of patients using lateral mass screws with a plating system, Heller et al.11 reported broken screws in 0.3%, screw loosening in 1.1%, and broken plates in 2.6% of their 78 patients. In the polyaxial screw-rod system, there have been no recent reports of screw hardware failure, including screw pull-out or loosening.14,23
In the reported series, lateral mass fractures have occurred in 6% of the Roy-Camille and 7% of the Margerl-directed screws.1 Katonis32 reported 14 (4%) lateral mass fractures of 356 screws, and screw pull-outs in two (3%) patients who had lateral screws with plate systems. As we previously mentioned, lateral mass fractures can be reduced by complete drilling and tapping of the entire premeasured length without skiving. In addition, to improve the overall postoperative stability of the area involved in the fusion including the bone graft, we recommend the following: 1) great care should be taken to not disturb the capsule at adjacent levels when the lateral masses to be fused are decorticated with the drill, 2) the medio-inferior side of the screw insertion point needs to be drilled to create a groove for the screw head, which will allow insertion of the entire premeasured length of the screw, 3) to preserve the kyphotic angle, it is helpful to tighten the screw nuts in a caudal to rostral direction to catch the rod.
In addition, computer navigational assistance and intraoperative somatosensory evoked potential (SEP) monitoring may become a valuable supplemental technique to minimize the complications of the posterior screw fixation system.
With an extensive knowledge of anatomy, polyaxial screw-rod fixation systems can be used safely with minimal complications for a range of cervical spinal diseases that require stabilization. The screw-rod system is more expensive than comparable plating systems. The advantages of this system over previous screw plate systems include the easy contouring of the rods, which prevents the risk of implant failure and loss of alignment, and the easy adaptation for extension to the occiput or thoracic spine. Although further studies are required to establish the long-term results in terms of fusion rates and clinical outcomes, the results from our study demonstrate the safety and efficacy of this system to date.


 XML Download
XML Download