

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Luteinizing hormone-releasing hormone (LH-RH) analogues are widely used for the treatment of prostatic cancer, myoma of the uterus, and central precocious puberty among other conditions. In Japan, two LH-RH analogues are available for the treatment of prostate cancer: leuprorelin acetate (LEUPLIN®, Takeda, Osaka, Japan) and goserelin acetate (Zoladex®, Astra Zeneca, London, United Kingdom). Both are marketed for 1- and 3-month use. These drugs can cause adverse reactions, such as hot flush, loss of libido, and osteoporosis. However, the occurrence of injection-site granulomas is rare. Although several reports of single cases of injection-site granulomas resulting from LH-RH analogues have been published, no case series has yet been described. Herein, we report 5 cases of injection-site granulomas induced by LH-RH analogues. In addition, we also describe the incidence rate of injection-site granulomas due to the administration of LH-RH analogues.
MATERIALS AND METHODS
We examined clinical records of prostate cancer patients who were treated in the department of Urology at Saga Prefectural Hospital, Koseikan, in 2005.
The LH-RH analogues leuprorelin acetate (used in 52 patients) and goserelin acetate (used in 66 patients) were administered to 118 patients. Androgen deprivation therapy by LH-RH analogues began in 33 of the patients in 2005. 11 of these were treated with leuprorelin acetate and 22 were treated with goserelin acetate.
Leuprorelin acetate was administered in the upper arm or abdominal wall, while goserelin acetate was administered in abdominal wall at an interval of 4-5 weeks (1-month use) or for 12-13 weeks (3-month use). While in Western countries leuprorelin acetate is administered intramuscularly and goserelin acetate is subcutaneously, in Japan both injections are administered subcutaneously.
RESULTS
In 5 of 118 patients, injection-site granulomas resulted from the administration of LH-RH analogues. The incidence rate was 4.2%. Furthermore all granulomas were caused by 11.25mg of leuprorelin acetate (5 of 47 patients, 10.6%). The patients' characteristics are summarized in Table 1.
Patient No. 1 was a 78-year-old man. He began androgen deprivation therapy with 3.75mg of leuprorelin acetate in August 2004. He received the last injection of 11.25mg of leuprorelin acetate in January 2005. Eight days later, he visited our department with complaints of a subcutaneous nodule and discharge at the injection-site. A pus specimen was bacteriologically negative. He was treated conservatively and the injection site healed within three months. Subsequently, he received an injection of 11.25mg of leuprorelin acetate at another site and then immediately visited the hospital with the same complaints as described above. As a result, his treatment was changed to goserelin acetate, and no further injection-site granulomas occurred.
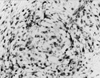
Patient No. 2 was an 82-year-old man. He began androgen deprivation therapy with 3.75mg of leuprorelin acetate in November 2004. He received the last injection of 11.25mg of leuprorelin acetate in December 2004. Two months later, he visited our department of dermatology complaining of a subcutaneous nodule at the injection-site. The nodule was resected and thereafter the wound healed normally. The nodule was histologically diagnosed as a granuloma (Fig. 1). Subsequently, he received an injection of 11.25mg of leuprorelin acetate at another site. Three weeks later, he visited with complaints of another subcutaneous nodule and discharge at the injection-site. A pus specimen was bacteriologically negative. He was treated conservatively and the injection site healed in about 3 months. Although his treatment was changed to goserelin acetate, the injection-site granuloma caused by leuprorelin acetate relapsed. The nodule was resected and the injection site healed. The histological findings were similar to case No. 1 (Fig. 2). Immunohistochemically, the observed inflammatory cells were mainly CD 3 positive T-lymphocytes and CD 68 positive histiocytes (Fig. 3 and 4). Finally, he underwent surgical castration.
Patient No. 3 was a 90-year-old man. He began androgen deprivation therapy with 11.25mg of leuprorelin acetate in January 2005. He received the last injection of 11.25mg of leuprorelin acetate in April 2005. Sixteen days later, he visited the department of surgery at our hospital complaining of a subcutaneous nodule at the injection-site. He was treated surgically and the wound healed normally. The histological findings indicated a granuloma. As a result, his treatment was changed to goserelin acetate, and no further injection-site granulomas occurred.
Patient No. 4 was an 86-year-old man. He began androgen deprivation therapy with 11.25mg of leuprorelin acetate in September 2004. He received the third and last injection of 11.25mg of leuprorelin acetate in May 2005. Four months later, clinicians noticed an asymptomatic subcutaneous nodule at the injection-site during a routine follow-up. Two months later, his tumor diminished without treatment. His treatment was then changed to goserelin acetate, and no further injection-site granulomas occurred.
Patient No. 5 was a 68-year-old man. He began androgen deprivation therapy with 3.75mg of leuprorelin acetate in 2002. He received the last and ninth injection of 11.25mg of leuprorelin acetate in April 2005. Three months later, clinicians detected an asymptomatic subcutaneous nodule at the injection-site during a routine follow-up. His tumor was resected and the wound healed. The histological findings indicated a granuloma. As a result, his treatment was changed to goserelin acetate, and no further injection-site granulomas occurred.
DISCUSSION
While injection-site disorders are rare, such reactions can cause a great deal of anxiety. Until now, injection-site granulomas have normally been associated with insulin and aluminum-containing tetanus toxoid vaccines.1 Injection-site granulomas resulting from the administration of LH-RH analogues were previously thought to be rare. Until now, only a few case reports have been published.2,3 However, we now report 5 cases (4.2%) of injection-site granulomas resulting from the administration of LH-RH analogues. In all cases, the injection-site granulomas were associated with administration of leuprorelin acetate, and in most cases, they occurred after the first or second administration of 11.25mg of leuprorelin acetate. The incidence rate was 9.6% (5 of 52 cases) when considering all administrations of leuprorelin acetate, and 10.6% (5 of 48 cases) when specifically considering the administration of 11.25mg doses. On the other hand, no injection-site granulomas were induced by goserelin acetate. Only one case (No. 2) had a relapse after the transition from leuprorelin acetate to goserelin acetate.
Why does leuprorelin acetate cause injection granulomas? Leuprorelin acetate is coupled with lactic/glycolic acid co-polymers or lactic acid polymers. Goserelin acetate is also coupled to lactic/glycolic acid co-polymers. The formation of granulomas could thus be related to such co-polymers, to polymers including the LH-RH analogue, or to the LH-RH analogue itself. It is likely that these granulomas were caused by delayed-type hypersensitivity to LH-RH analogue injection, as indicated in Fig. 3 and Fig. 4. The difference in the incidence rate may be due to differences in immunogenicity between leuprorelin acetate and goserelin acetate. It is possible that leuprorelin acetate is a stronger immunogenic agent, preventing us from using other LH-RH analogues such as goserelin acetate. Furthermore, the long-acting 11.25mg dose of leuprorelin acetate may more easily induce a delayed-type hypersensitivity as compared to the fast-acting 3.75mg dose, because all 5 of granulomas were associated with this type of leuprorelin acetate. We hypothesize that there are three possible mechanisms for this difference. The first is the difference in molecular weight of polymer substrate. The polymer substrate of the long-acting form has larger molecular weight than that of fast acting treatment. Second and third, the difference in drug amount and effective (or toxic) period may explain the observed results. These three possible mechanisms may lead to injection-site granulomas to different degrees.
Granulomas resulting from the administration of leuprorelin acetate have rarely been reported in Western countries. However, several reports have been published in Japan. The reason for the difference in incidence rate between western countries and Japan may depend on the method of injection. While leuprorelin acetate is administered intramuscularly in Western countries, it is injected subcutaneously in Japan. These results suggest that injection-site granulomas result from shallow injections.4 Therefore we think that changing the method of administration from subcutaneous to intramuscular injections may resolve this problem.
Saxby indicated that injection-site granulomas resulting from the administration of an LH-RH analogue may be more common than previously thought.3 In our study, the incidence rate was unexpectedly high (4.2%). This phenomenon thus seems to be a serious problem since patients with this adverse reaction must change their therapeutic regimens, moving to another LH-RH analogue or undergoing surgical castration, for instance.
Goserelin acetate may cause fewer granulomas than leuprorelin acetate. However no definite treatments exists once granulomas develop. There are also no predictable measures of this problem. We should therefore keep in mind that the LH-RH analogues may cause injection-site granulomas at a rate as high as a 4.2%, when considering all LH-RH analogues, or as high as 9.6% when only considering the use of leuprorelin. Such patients have very limited therapeutic options.
Until now, the occurrence of granulomas due to the administration of LH-RH analogues was thought to be rare. However, our study revealed a higher incidence rate than expected, especially after the administration of leuprorelin acetate. Such a reaction can cause a great deal of anxiety to patients. Urologists need to be aware that such reactions can occur and take care when using LH-RH analogues, especially when using leuprorelin acetate.


 XML Download
XML Download