

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Health system planning is a challenging task, which tends to be exacerbated by a lack of detailed information on practice variations across regions and demographic characteristics. One of the major barriers to coherent, effective health policy is, simply, that often very little is known about the characteristics of private-sector clinics and their performance. That data is crucial in the structuring of effective policies.1 There is a clear consensus that we require more information than simple head counts of physicians. We need to ascertain, for example, differences in productivity according to such disparate factors as the sex of the physician, the competitive state of clinics, the income elasticity associated with clinics productivity, how the clinic responds to differences in age demographics over time, etc. This information would also help policy makers to design and introduce mechanisms for the effective monitoring and regulation of this sector.
However, there is currently a dearth of studies addressing the productivity of private clinics, largely due to the paucity of accurate financial data, which is often a managerial secret in private-sector clinics of developing countries. Recently, a study assessed the productivity of Canadian family physicians, but that study simply described distributions of productivity according to general characteristics, not by controlling the confounding variables.2 Productivity, with respect to trends and determinants, has been investigated in America, but most of that has been cross-sectional results from one-shot studies.3-5
With respect to developing countries, the determinants of private physicians productivity in Macedonia have been studied, but the study utilized sampled self-reported data.6 Likewise, the characteristics of Indian physicians were studied, but that study failed to assess productivity.
Therefore, we attempted to evaluate the determinants of private clinics' productivity in South Korea, and compared city and county clinics using National Health Insurance panel data, collected from 9,212 private clinics, from 1996 to 1999. Since the study population covers all the private clinics of solo practitioners in Korea, except for those who opened or closed their practices during this period, the findings from this study constitute a nationwide analysis of the determinants of private clinics' productivity.
MATERIALS AND METHODS
Subjects
We analyzed every private clinic in Korea which submitted insurance claim data to the Korean National Health Insurance Corporation (KNHIC) from 1996 through 1999, after excluding clinics that opened or closed during the study period, or where more than two physicians worked, or the specialties whose percent over the total clinics were less then 1% as like thoracic surgery, plastic surgery, anesthesiology, pathology, et al. The number of private clinics excluded in final analysis was 1,150 clinics. This exclusion was made to ensure the homogeneity of data. Therefore, four years of panel data (36,876), from 9,212 clinics, were made available to our study. The clinics' revenue and characteristics were obtained from the KNHIC. Regional socio-economic characteristics were obtained from the yearbook published by the Korean Statistical Bureau, and the local governments.
Statistical analysis
Variables were analyzed via Student's t-test, ANOVA, and correlation analysis, by region and year. We also conducted a multivariate analysis, in order to control for the effects of confounding variables. However, a multiple regression analysis by ordinary least square (OLS) could not be employed in this study, as the study data was repeated measures data, meaning that it did not meet the independence assumption necessary for OLS. Moreover, the randomized block design for repeated measures data could not be used here, because all observations within the blocks could not be correlated equally. Accordingly, we used the mixed model, with a special parametric structure of covariance matrices.7 Among the simple, compound symmetrical, first-order autoregressive, and unstructured models of covariance, we chose unstructured covariance as the covariance structure of our model. This was due to the observation that the AIC (Akaike's Information Criterion) and the SBC (Schwarz's Bayesian Criterion) scores would be the lowest in the unstructured model. This analysis was performed according to the PROC MIXED procedure, detailed in SAS version 8.2. For comparisons of other countries, and the normal distribution statistical assumption, we transformed the dependent variable and income variables by natural log. Thus, the coefficient estimate was interpreted as the rate of change in the log form model, and was interpreted as elasticity in the log-log form model.
Variables
The dependent variable was the annual revenue from 1996 through 1999. This revenue data was adjusted to the present value of the year 1996, using an annual increase rate in the fee schedule (i.e. 8.15% in 1997, 7.68% in 1998, and 3.90% in 1999).8
The independent variables included each physician's sex, age, and specialty, number of beds, and region in which the clinic was located, number of clinics and beds per 100,000 persons, inhabitants incomes, and proportion of elderly in the unit in which the clinic was located. Although controlling natural trends via the mixed model, we also controlled for the effects specific to the year, most notably the 1997 Asian crisis, by using dummy variables.
The administrative units were assessed by city for small cities, county for rural areas, and district for large cities. This method is generally consistent with the living zones of Koreans. Inhabitants' incomes were evaluated by inhabitant tax per capita, and this value was adjusted by the inflation rate. The region of the clinic was determined in terms of city or county.
RESULTS
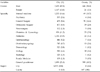
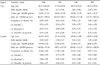
The percentage of male physicians was 87.0% in cities, and 96.8% in counties; the percentage of general practitioners was 21.0% in cities and 60.3% in counties (Table 1). In cities in 1996, the mean of physicians' ages was 46.7 years; mean number of beds per 100,000 persons in the administrative unit was 401.7 beds; mean of revenue, transformed by natural log, for clinics was 4.92. In rural areas in 1996, the mean of physicians ages was 46.2 years; mean number of beds per 100,000 persons in administrative units was 168.2 beds; mean revenue, transformed by natural log, for clinics was 5.26 (Table 2).
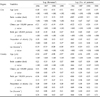
For male physicians, revenue and number of patients, transformed by log, were significantly higher than that of female physicians, in both city and county from 1996 to 1999. Revenue and number of patients, transformed by log, also exhibited significant differences according to the specialty of the physician, in both city and county from 1996 to 1999 (Table 3, 4).
The age of the physician was significantly negatively associated with revenue and number of patients, transformed by log (Table 5). The number of beds was significantly positively associated with those variables. The number of clinics and the number of beds per 100,000 were significantly negatively associated with revenue and number of patients in city clinics, but there was no such significant trend observed in the counties. The proportion of elderly patients was positively associated with revenue and number of patients, in both cities and counties. The income of the administrative unit was significantly negatively associated with the revenue and number of patients for clinics in the city, but was positively associated with those variables in county clinics, with the exception of revenue in 1998.
The results of the multivariate analyses for revenues and number of patients, transformed by log, are listed in table 6. Our results showed that those factors were significantly negatively associated with age; significantly positively associated with number of beds; were significantly different according to the specialties and sex of the physicians; and were significantly positively associated with the proportion of elderly patients, in both city and county clinics. But the number of clinics and beds per 100,000 was significantly negatively associated with those variables, and the income of administrative units was significantly associated with the revenue and the number of patients only in the city. Number of patients and revenue in 1997 were significantly higher than in 1996, but in 1998 and 1999 were significantly lower than in 1996.
DISCUSSION
The results of the multivariate analysis in this study showed that the productivity of clinics was significantly negatively associated with the age of the physicians. It was reported that younger physicians used more clinical tests,9 because younger physicians were more apt to depend on clinical tests, and older physicians were not as familiar with the clinical tests.10 Previous studies of Korean physicians also reported a negative association of productivity with the age of the physicians.11-13
In this study, the number of patients and the revenue of the male physicians were significantly (27-77%) higher than that of female physicians. Notably, revenue of male physicians was 77% higher than that of female physicians in the counties. It has been reported previously that the productivity of male physicians was greater than that of female physicians.2,3,13
All other things being equal, one more bed per clinic was reported for every 1.2-1.6% significant increase in revenue and 0.7% significant increase in number of patients. Differences in coefficients by region were trivial.
The number of clinics per 100,000 was negatively associated with revenue and number of patients, but this was significant only in the city. These results were presumably due to the degree of competition. The number of clinics per 100,000 in city was 31.09, but in the county, that value was only 19.99 in 1996.
One more bed per 100,000 was reported for every 0.003-0.004% significant decrease in revenues and number of patients, and a 1% income increase was reported for every 0.01% significant decrease in the number of patients, only in the city. The rates of change for the number of beds per 100,000 and the income elasticity in the county were smaller than those found for the city, and were not significant. These results were presumably due to the substitution effect of hospital services for clinic services and income effect.14 The National Health Insurance System of Korea constitutes social insurance, covering the entire Korean population, including all medical institutions. Clinics should compete with hospitals, because hospitals have big outpatient departments, offering primary care services. But beneficiaries should pay 30% of total outpatient care expense in clinics, and 45% to 50% of total outpatient care expenses in hospitals. As a result of co-payment, the ratio of outpatients to inpatients in the metropolitan hospitals located in relatively high-income areas was 2.2, but in non-metropolitan hospitals, it was 1.7.15 Therefore, with increasing income, it appears that the substitution effect, using more hospital services and less clinic services, may be more pronounced than the income effect, using more clinic services in the city where income is higher then in the county. In the county, where incomes are generally lower than in the city, the substitution effect may be fairly similar to the income effect.
The proportion of elderly patients was significantly positively associated with both revenue and number of patients. It has been generally accepted that the elderly use more medical services.16-19 As might be expected, both number of patients and revenue decreased after 1998, the year after the Asian Economic Crisis, which occurred in December, 1997.
Our study contributes to a further understanding of the determinants of private clinics productivity. First, every private clinic in Korea was analyzed for the determinants of productivity. Since 97% of the Korean population is covered by National Health Insurance and the remaining 3% are covered by Medicaid,20 the revenue data obtained from the KNHIC for this study accurately represents the actual revenue resulting from reimbursement to all medical institutions in Korea. Second, we analyzed determinants of the revenue and the number of patients for clinics' productivity separately, in order to better understand the possible influences of case-mixing. Third, we analyzed four years of panel data in order to control the natural increasing trends using the mixed model. Finally, we controlled for various confounding variables, using the mixed model.
This study is not without its limitations. First, while several independent variables were assessed in this study, variables such as paramedics, marketing strategy, the reputation of medical specialists, the introduction of high cost medical equipment, etc. may also have influenced financial performance.
For example, while this study reports differences in productivity according to the sex of the physician, Dedobbeleer et al.21 reported that differences in productivity according to the sex of the physician were decreasing with increases in the working hours of female physicians, and with the female physicians' assumption of the habits and behaviors of male physicians. Others5,11,12,20 have reported that differences in the number of patients, revenue and income, according to the sex of physicians, were not significant, after controlling for medical equipment and paramedics. Therefore, sex-mediated differences, etc. found in this study might actually be confounding effects, predicated on differences in the acquisition of medical equipment and paramedics.
Second, our results don't represent whole clinics in Korea, because this study excluded 1,150 clinics that opened or closed during the study period, or where more than two physicians worked, or the specialties whose percent over the total clinics were less then 1% for the homogeneity of data. So, the generalization of our results for the general clinics needs caution.
As to provide more useful data for structuring effective policies, the future research are needed to identify effects of our omitted variables such as paramedics, marketing strategy, the reputation of medical specialists, the introduction of high cost medical equipment, etc. may also have influenced financial performance, and to investigate the productivity of clinics where more than two physicians worked and minority specialties clinics.



 XML Download
XML Download