

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Duplications of the alimentary tract are rare congenital anomalies. Although the duplication can occur along any part of the alimentary tract,1 the hindgut is rarely affected. In a review of 8 series, where 495 alimentary tract duplications in 455 patients were studied, Stringer et al.2 found that only 7% of the duplications involved the colon. The transverse colon is a relatively uncommon site of duplication in the hindgut.3
Most duplications of the alimentary tract are symptomatic and are thus detected and treated in infancy or childhood. However, some lesions are unrecognized until adulthood because the signs and symptoms caused by the duplications are vague, making correct interpretation of the clinical findings difficult.
Upon review of the Korean literature, one case of tubular duplication of the transverse colon was reported in a 9-year-old female.4 To our knowledge, this paper is the first report of a tubular duplication of the transverse colon in an adult in Korea.
CASE REPORT
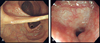
A 40-year-old woman was referred to the Colorectal Section, Department of Surgery, Yonsei University College of Medicine, Seoul, Korea on February 23rd 2004 because of findings on an abdominal CT scan was taken for routine health check-up at a local community hospital, which showed a 8 × 3 cm sized cystic mass in the right lower quadrant. She did not complain of any gastrointestinal symptoms including pain, nausea, vomiting, or bowel habit change, and denied any history of melena or hematochezia. On physical examination, there was no palpable mass or tender area in the abdomen. Laboratory study findings were within normal limits. Barium enema revealed tubular duplication of the transverse colon (Fig. 1A). The duplicated segment originated from the lateral border of the mid ascending colon about 7 cm distal from the ileocecal valve and ended inferior aspects of the transverse colon just proximal to the splenic flexure, running parallel to the transverse colon and communicating at both ends (Fig. 1B). Colonoscopy demonstrated a normal colonic mucosa in the duplicated segment (Fig. 2A). The lumen of the duplicated segment was similar in diameter to the transverse colon at the distal opening, but gradually narrowed proximally. The colonoscope could not be passed through the proximal opening of the segment (Fig 2B). The patient did not require any treatment and has been doing well without complaints during a follow-up period of 4 months.
DISCUSSION
Duplications of the alimentary tract are spherical or tubular structures, which possess a well-enveloped smooth muscular layer lined with the mucosa,5 which may be blind or communicating with the proper lumen. The shapes of duplications are more commonly spherical rather than tubular. Tubular duplications usually communicate with the adjacent bowel and the symptoms may vary according to the presence of their proximal and distal communications.6 In this patient, the duplicated segment was communicating with the normal transverse colon at both ends. It is likely that the stool and mucus had been freely passing into the duplicated segment since there were no symptoms.
The pathogenesis of these lesions has not yet been well characterized. One of the most widely accepted theories is that an abnormality of the embryonic gut results in the formation of a diverticulum, a cyst, or twinning of a bowel segment.7 Environmental factors such as trauma or hypoxia during early fetal development have also been suggested to play a role.8
Symptomatic or complicated duplications, including bowel obstruction, perforation, and malignancy are indications for surgical resection, but the lesion is not appeared to contribute to the symptoms, surgical correction is unnecessary for asymptomatic lesions.9
The patient described in our report presented with the above clinical characteristics reported in the literature. The patient presented with no symptoms and a mesenteric cyst was initially suspected from abdominal CT scan. Barium enema and colonoscopy made the definitive diagnosis by demonstrating a tubular duplication of the transverse colon and the patient did not require any treatment after the diagnosis.
Although duplications of the alimentary tract are rare, the possibility of congenital lesions of the alimentary tract should not be overlooked even in adults presenting with vague or no gastrointestinal symptoms.

 XML Download
XML Download