

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
In a literature search, there are more than 20 reports of skin metastasis from transitional cell carcinoma (TCC) of the bladder and only 3 from pelvic cancer.1 Metastasis to the abdominal wall of bladder carcinoma results mainly from iatrogenic seeding.2,3 Otherwise, primary metastasis to the abdominal wall of TCC is accepted as a late manifestation of systemic spread.4,5 This paper describes a case of late metastasis to the abdominal wall without skin involvement of TCC in a 66-year-old woman. To our knowledge, this is a rare case of bladder cancer with metastasis to the abdominal wall after the longest time span.
CASE REPORT
A 66-year-old woman presented to the outpatient clinic with a 10-month history of skin lesion. She had undergone radical cystectomy with ileal conduit 20 years prior at our institution. At that time, histopathological examination had revealed well-differentiated (WHO grade I/III), muscle invasive TCC with a staging of cT2N0M0. After discharge, she had attended intermittent follow-up visits.
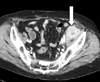
On the present admission, her vital signs were stable and physical examination revealed a mass, which was hard and tender, 8 cm in diameter, and located in the right inguinal area. Physical examination revealed another palpable mass in the left lower abdomen. Her past medical history was unremarkable. Laboratory data were within normal limits. Clinical staging with computed tomography showed one mass with several calcifications in the left lower abdominal wall and an additional mass in the right inguinal area (Fig. 1), and but no abnormal findings in other organs. Chest x-ray and bone scan were clear.
A wide excision of the masses in the left lower abdominal wall and right inguinal area was performed and skin flaps were used for skin coverage. The surgical specimens revealed well-differentiated TCC (Fig. 2). She subsequently underwent two postoperative cycles of combination chemotherapy with gemcitabine and cisplatin. However, follow-up computed tomography revealed that a new lesion had developed in the pelvic cavity (Fig. 3). Another chemotherapy regimen of methotrexate, vinblastine, doxorubicin and cisplatin (M-VAC) was advised. At the time of writing the results of this second treatment were not conclusive.
DISCUSSION
Several cases of metastasis to the abdominal wall of TCC have been reported previously. Seeding of TCC outside the urinary tract often occurs after iatrogenic procedures, such as partial cystectomy, suprapubic cystectomy, pyelotomy and laparoscopy.2,3 Because metastasis to the abdominal wall is rare, some authors regarded it as a late manifestation of systemic spread.4,5 Spector et al. suggested that skin metastasis in TCC was the result of increased longevity in successfully treated patients.4 In addition, skin metastases have been one aspect of diffuse metastatic disease developing often with multiple organ sites involved.
Abdominal wall metastasis of TCC of the urinary tract may be an ominous sign, such a lesion should be assessed as a part of overall staging, and systemic chemotherapy is a possible therapeutic option which should be considered.6 However, although some cases responsive to systematic chemotherapy have been reported, this metastasis usually portends a rapid progression of the disease and poor prognosis.7 Urologists should carefully evaluate patients with soft tissue metastasis with the aim of diagnosing any associated malignancy, particularly bladder cancer.
In our patient, the pathological process seemed to be a result of hematogenous or lymphatic metastasis, rather than multicentricity or implantation, since the tumors were localized within soft tissues without skin involvement. Thus, the masses were diagnosed as metastasis of bladder cancer due to their clinical and histological findings. Their characteristic features included no other metastatic lesion of the skin and no recurrence of the tumor during 20 years after cystectomy. In summary, we report what appears to be a unique case of TCC of the bladder with abdominal wall spread over a time span of 20 years of a locally invasive tumor or of the other sites of dissemination.


 XML Download
XML Download