

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Lipofibromatous hamartoma is a rare benign tumor in which the fibrous and fatty tissues gradually proliferate into the major nerves and their branches in the body. It is believed to be congenital and mainly affects the median nerve in the hand. However, this tumor rarely affects the digital nerves at the peripheral level. It is mainly seen in young adults and its natural course is self-limiting. Nonetheless, surgical treatment may be needed when the tumor becomes large or begins to compress a nerve. We encountered a patient with this benign tumor that symmetrically affected the digital nerves in both hands, and thus, for the first time we report this case along with the review of the literature.
CASE REPORT
A 22-year-old woman visited the outpatient clinic at our hospital presenting protruding lesions that had been gradually growing on the index fingers of both hands. Her chief complaint was, in her words, that there was hyperkeratinized skin on both index fingers and she wanted to remove the hyperkeratinized skin esthetically. She had been working as a typist for the past 2 years and had reported that the lesions have grown for 2 years. Physical examination showed 1 × 2 cm subcutaneous masses on the ulnar sides of the proximal interphalangeal joints, but no sensory symptoms or motion limitation were present. At the time of surgery, the masses with much fat content were discovered in the digital nerves on the ulnar sides. With the aid of a microscope, an intraneural microdissection was performed aiming at removing as much of the mass as possible without sacrificing the major nerve branch. In order to preserve sensory function, we had to leave some part of the mass that was severely adherent to the main digital nerve. We thought that the mass might be infiltrating hyperkeratinized skin. Therefore, we have performed an excision of the mass with skin and a direct closure of both skin margins. The surgical outcome was satisfactory in the esthetic aspect and no sensory dysfunction or evidence of recurrence was found during the 15 months of postoperative follow-up.
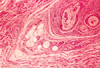
Histologic results showed the masses to be lipofibromatous hamartoma that originated from the digital nerves. There was no invasion of the surrounding tissues. Immunohistochemistry, which was performed additionally, was positive for CD34, S-100 protein, and vimentin, and was negative for epithelial membrane antigen (EMA), desmin, and glial fibrillary acidic protein (GFAP) (Fig. 1, 2, 3, 4, 5).
DISCUSSION
Lipofibromatous hamartoma (neural fibrolipoma) is a rare benign tumor that gradually proliferates into the fibrotic and fat tissues by infiltrating major nerves and their branches.1 This tumor is congenital in nature, frequently affects the median nerve of the hand, and is commonly related with macrodactyly.2,3 Macrodactyly is associated with approximately one-third of lipofibromatous hamartoma in the upper extremities, with an incidence of 0.5 per cent of all anomalies of the hand.4,5
Lipofibromatous hamartoma is mainly seen in young children and adults and affects the sensory territory of the median nerve, in which case, this tumor expands from the median nerve trunk to the common digital nerve and further down to the peripheral digital nerves in most cases. There have been some reports that observes lipofibromatous hamartoma affecting the radial nerve and ulnar nerve, respectively.6,7 This tumor frequently affects the peroneal nerve in the lower extremities. However, it was reported that this tumor rarely affects the digital nerves in the peripheral region. Moreover, there have been no reported cases indicating that it affects both hands symmetrically. According to the reference, lipofibromatous hamartoma that involves the digital nerve develops mostly on the dominant hand (mainly Rt. hand). A remarkable factor in this case is that the patient's occupation was a typist. We came to a conclusion that repeated loading of minor trauma on both hands may be a factor for symmetric occurrence of the tumor on bilateral digital nerves.
Lipofibromatous hamartoma is usually diagnosed as a fat-containing soft tissue mass on the CT or MRI.8 Differential diagnosis is needed to exclude lipoma, lipofibrous hamartoma, lipoblastoma, lipomatous hibernoma, hemangioma, elastofibroma, and liposarcoma as possibilities. Although a histologic test is needed to determine whether the tumor is malignant or benign, it has been reported that fine needle aspiration biopsy is not sufficient for definite diagnosis.
Microscopic findings of lipofibromatous hamartoma usually reveal abundant fatty and fibrous tissue going through the nerves. In the subcutaneuos tissue, the fat has the appearance of a yellow, well-located, adult storage fat. In the involved nerves, there is a marked fatty infiltration between the fasciculi, with fibrotic thickening of the endoneurium and perineurium. Unlike lipoma, it shows an infiltrative pattern. It was reported that this tumor is positive for CD34, S-100 protein, neuron-specific enolase, and vimentin according to the immunohistochemistry.4 As reported in other studies, we also found that the tumor was positive for CD34, S-100 protein, and vimentin, which means that its fibro-fatty tissue may originate from the endoneurium.4
There is no standard treatment yet, and different opinions have been reported on the treatment of this tumor. If this tumor is related with macrodactyly, it is usually treated with surgery since overgrowth of the skeletal system is usually involved when present in young children.
When it is present in young adults, it possibly goes through a self-limiting course since the growth of this tumor is very slow. Some authors have reported that the size of this tumor decreases naturally when left untreated.2,9-11 There has been no case report on a malignant case of lipofibromatous hamartoma. Therefore, conservative treatment on a long-term basis should be emphasized.
However, surgery may be required when the tumor is large enough in size or compresses a nerve. The preservation of major nerve branches is important at the time of surgery. Clinicians need to avoid radical resection that sacrifices major nerve branches since this risk can not be avoided even with the introduction of microscopic surgery due to possible ischemic complications of the nerve.3
We experienced a rare case of benign lipofibromatous hamartoma affecting the digital nerves in both hands. The shape of the hand improved only with partial excision. This patient displayed fair outcome after surgery, presenting no specific nerve complication and no evidence of recurrence. According to the literature review, this is the first case report of lipofibromatous hamartoma that affected the digital nerve of both hands symmetrically.




 XML Download
XML Download