

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Imaging modalities like computed tomography (CT) and magnetic resonance (MR) imaging rely on detecting anatomic changes for the diagnosis, staging and follow-up of cancer patients. However, positron emission tomography (PET) has the ability to demonstrate abnormal metabolic activity, and 18F-2-deoxy-D-glucose (FDG) PET provides important tumor-related qualitative and quantitative metabolic information that may be critical for the diagnosis and follow-up (1-3). Moreover, the combination of PET and computed tomography (PET/CT) allows the functional PET and anatomical CT images to be acquired under identical conditions and then they are rapidly co-registered. This combined system has advantages over CT alone as functional information is added to morphological data, and this combined system has advantages over PET alone because pathological areas of tracer uptake are better localized and the image acquisition time is reduced (4-7). Moreover, the limited specificity of PET that's due to the increased glucose metabolic activities of benign tumors and inflammatory tissues (such as those of tuberculosis) can be partially overcome by PET/CT (8, 9).
In this study, we investigated the role of PET/CT for evaluating breast cancer.
PATIENT SELECTION
Fifty-eight female patients with known breast cancer (age range: 34-79 years old, mean age: 50 years), and who underwent PET/CT examinations at our facility between April 2003 and June 2005 were enrolled in this study. The PET/CT examinations were performed for the initial tumor staging, for suspected recurrence after breast operation and for follow-up after chemotherapy.
PET/CT IMAGING
Whole-body PET/CT imaging was performed using a combined PET/CT scanner (Gemini, Philips Medical Systems, Bothell, WA). The Gemini is an open PET/CT system that combines a helical dual slice CT scanner and a 3D PET scanner equipped with its own transmission source. The MX8000 EXP CT scanner is a dual slice system with a detector that consists of 1,344 cadmium tungstate elements. After having the patients fast for at least four hours, they were administered an intravenous injection of 240 to 400 MBq (approximately 10 mCi) FDG; oral contrast was not administered. The blood glucose levels were checked in all the patients before FDG administration, and no patient had a blood glucose level that exceeded 200 mg/dl. The CT images were acquired from the cerebellum to the pelvis without intravenous contrast media, and a whole-body emission PET scan was performed for the same axial coverage. The PET, CT and fused PET/CT images were generated and then reviewed on a computer workstation.
ROLE OF PET/CT
Primary Tumor
The ability of PET to detect breast cancer depends on the tumor's size and histology. The sensitivity of PET has been reported to be 68% for small (< 2 cm) tumors and 92% for larger (2-5 cm) tumors (10), and its reported overall accuracy for detecting in situ carcinomas is low (sensitivity: 2-25%). The major limitation of PET or PET/CT for breast imaging is its poor detection rate for small breast carcinomas and non-invasive breast cancers (Fig. 1).
However, PET/CT has a role to play in a selected group of patients, such as those with dense breasts or with implants, for determining tumor multiplicity, for localizing the primary tumor in those patients with metastases of a breast origin when the mammography is indeterminate, and for those patients whom biopsy is not a desirable option (11, 12). PET/CT has a potential advantage over PET for evaluating small lesions in which the uptake may be artifactually lowered due to the partial volume effect of PET because areas of mild hyperglycolytic activity can be reliably assigned to normal or abnormal anatomical structures (Fig. 2).
Regional Lymph Node Metastasis
Axillary lymph node metastasis is an important factor when determining the prognosis of patients. Breast cancer patients with four or more involved axillary lymph nodes have a significantly higher risk of recurrence (13). The sensitivity and specificity of axillary PET imaging in breast cancer patient have been reported as 79-94% and 86-92%, respectively (11, 14). PET/CT can accurately localize and differentiate the metastatic and reactive lymph nodes when CT shows multiple enlarged lymph nodes in the axilla (Fig. 3).
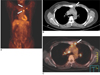
The metastasis to the internal mammary or mediastinal lymph nodes in breast cancer patients is often clinically occult. The prevalence of abnormal findings for the internal mammary or mediastinal lymph nodes by PET was about twice than of conventional CT in those patients with recurrent or metastatic breast cancer (15). In a study by Tatsumi et al., although the sample number was small, PET/CT appeared to be more useful than CT for evaluating the internal mammary and mediastinal lymph nodes because the smaller lymph nodes sometimes produced equivocal or negative CT findings (7) (Fig. 4).
Distant Metastasis
Distant metastases from breast cancer are frequently found in the lungs, liver and bones. One advantage of whole-body PET imaging over conventional imaging modalities such as chest films, bone scanning, and abdominal ultrasound is its ability to detect metastasis at different sites and organs during a single examination (Fig. 5). Moon et al. found that whole-body PET imaging had high diagnostic accuracy for patients with suspected recurrent or metastatic breast carcinoma (16). Based on the number of lesions, its sensitivity for detecting distant metastasis was 85% and its specificity was 79%.
Cook et al. found that PET was superior to bone scintigraphy for detecting osteolytic breast cancer metastases (17) (Fig. 6). In contrast, the osteoblastic metastases showed lower metabolic activity and they were frequently undetectable by PET (17, 18). Yet PET/CT can overcome this limitation, and osteoblastic bone lesions, even if negative on PET scans, can be identified on CT images (Fig. 7).
Treatment Monitoring
To downstage primary tumors prior to surgery and to abolish occult distant metastases, neoadjuvant chemotherapy is now being increasingly used to manage patients with large and locally advanced breast cancer. Moreover, several studies have demonstrated that patients with unresponsive tumor may achieve improved survival by administering alternative chemotherapy and/or prolonged courses of chemotherapy (19, 20). Considering the side effects of chemotherapy, there is a need to quickly identify the non-responding patients early in their treatment.
At present, the anatomical imaging modalities are commonly used to evaluate the response to treatment by evaluating the changes of the tumor's size. Nevertheless, sequential measurement of tumor size frequently does not allow the determination of early response. The effect of PET for evaluating the response to treatment has already been demonstrated for different types of neoplasm, including breast cancer (Fig. 8). In a study by Smith et al, the mean reduction in FDG uptake after the first cycle of chemotherapy was significantly higher in the lesions that showed a partial (p = 0.013), complete macroscopic (p = 0.003), or complete microscopic (p = 0.001) response than that of the non-responsive lesions, as determined by histopathological examinations (20). Rose et al. have reported that after a single cycle of chemotherapy, PET predicted the complete pathological response with a sensitivity of 90% and specificity of 74%, and by using a decrease of FDG uptake at the threshold of < 55%, as compared with the baseline scan, all the responders were correctly identified after the first treatment course (100% sensitivity and 85% specificity) (21).
PET/CT may also play a role in radiation therapy planning by providing an accurate estimate of the extent of tumor (22).
Recurrence
Detecting early recurrence has an important survival benefit because it prompts clinical consideration for administering different therapies. However, it is difficult to differentiate true recurrence from postsurgical sequelae and radiation sequelae with using just the conventional imaging modalities. Locoregional recurrences predominately affect the breast, skin, the axillary and supraclavicular nodes, and the chest wall (23, 24).
Grahek et al. studied 134 patients with suspected recurrence and they found that the sensitivity and specificity of PET for detecting recurrence were 84% and 78%, respectively, whereas the sensitivities and specificities of the conventional imaging modalities were 63% and 61%, respectively (25). PET is considered to be highly effective for evaluating patients with suspected recurrent breast cancer, and it surpasses the other conventional imaging modalities in terms of whole-body evaluation. The CT data from a PET/CT examination allows the appropriate anatomical localization of foci of FDG uptake (Fig. 9).








 XML Download
XML Download