

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Neurofibromatosis type 1 (NF-1) is a relatively common autosomal dominant disorder that occurs in one in 3,000 live births. It is a hamartomatous disorder that originates in the neural crest and is characterized by neural tumors, cafe-au-lait spots, and Lisch nodules. Skeletal signs include scoliosis, sphenoid wing dysplasia, bony distortion and local cystic and erosive change. Although sphenoid wing dysplasia has been observed in between seven to 12.8 percent of patients with neurofibromatosis, the absence of a sphenoid wing is very rare (1-3). We report here an unusual case of NF-1 with an associated absence of a sphenoid wing by using multidetector computed tomography (MDCT).
CASE REPORT
A 31-year-old white man was admitted to our hospital with complaints of severe head pain and cross-eyed right globe. Physical examination revealed a normotensive man with cafe-au-lait spots on his chest and abdomen (Fig. 1). An ophthalmic examination revealed that his vision was normal except his right cross-eyed towards out paralysis and enophthalmos. Another notable finding was the discovery of a family history of neurofibromatosis. The patient was accepted for radiological evaluation in our clinic. MDCT was performed using an Aquilion scanner (Toshiba Medical Systems, Tokyo, Japan) with 16 high-resolution detectors. The images were obtained to define the caudocranial extent of the neck to the head region, by using a collimation of 1 mm×16 rows, with a helical pitch of 3, a gantry rotation speed of 0.75 sec per round, voltage of 120 kV and current of 300 mA. Three-dimensional images were reconstructed using maximum intensity projection (MIP) and 3D rendering algorithms on a Vitrea 2 (Vital Image Inc) workstation.
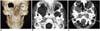
The anterior volume rendered 3D CT image showed details of a bony defect in the right orbital region (Fig. 2A). Thick multiplanar axial reconstructions (MPR) revealed the absence of the right sphenoid wing, and the intracranial and orbital contents were separated only by dura mater (Fig. 2B). In addition, the transverse bone window MDCT scan, performed at the level of the orbit, revealed the absence of the right sphenoid wing, right eye microphthalmos, increased fat tissue in the retrobulbar space and an enlarged middle cranial fossa. Furthermore, the left globe was larger than the right (Fig. 2C).
DISCUSSION
Neurofibromatosis type 1 may affect all systems of the human body. It is a hamartomatous disorder that originates in the neural crest and secondarily affects the supporting mesenchyme. The disorder, which is characterized by pigmented cutaneous lesions and generalized tumors that originate in the neural crest (taking the form of a discrete fibroma nodule or a plexiform neurofibroma), manifests itself in various ways. Central nervous system indicators consist of an increased incidence of astrocytomas, meningiomas, schwannomas, and ependymomas. Other features of the disease include bony dysplasias, kyphoscoliosis, sphenoid wing hypoplasia and vascular dysplasia. Sphenoid dysplasia is one of the characteristics of NF-1, occurring in 5-10% of cases. Furthermore, abnormalities of the sphenoid wings are often considered pathognomonic. However, complete dysgenesis of the sphenoid wing is very rare (1-4). Its radiological characteristics describe the area of defect in the greater sphenoid wing and enlargement of the middle cranial fossa. Many ophthalmic manifestations may occur in NF-1 patients. Lisch nodules are virtually all pathognomonic, and Huson et al. (5) found these iris hamartomas to be present in all of his NF-1 patients over the 16 years of age. Other ophthalmic findings include choroidal hamartomas, plexiform neurofibromas, retinal phakomos and optic nerve gliomas. Exophthalmos and enophthalmos, potential sequelae, are associated with orbital tumors and/or sphenoid wing dysplasia (1, 6).
Unilateral enophthalmos, primarily viewed as a complication of an orbital fracture, may result from other causes such as microphthalmos, orbital fibrosis, and sclerosing orbital tumors (1, 3). Congenital microphthalmia occasionaly accompanies sphenoid dysplasia or similar sphenoidal abnormalities. The neuro-ophtalmological findings of NF-1 are variable, pulsating exophthalmos is a common one. However, in a few cases in which NF-1 patients have sphenoid dysplasia, enophthalmos was also seen as a result of microphthalmia or because the lateral wall of the orbit was deficient and allowed decompression of the neurofibromatous tissue or retrobulbar fat into the temporal fossa (7). The present case had NF-1 with sphenoid wing dysgenesis leading to enophthalmos, but neurofibroma was not observed.
The recent development of MDCT, which can quickly scan a large longitudinal area and enable us to obtain thinner section collimation within a short period of time, allowed us to obtain isotropic volume data for 3D imaging. The volume data obtains serviceable 3D images by using various reconstruction methods such as high-quality MPR, MIP algorithm, surface rendering and volume rendering. Sixteen-slice scanners can shorten the duration of scanning as well. By using thick MPR techniques, image quality can be improved while keeping patient dose low. Reconstructing overlapping thin-section data provides the basis for image reconstruction in any desired plane. Proper reconstructions, 3D images and postprocessing allow better visualization of structures and their normal and abnormal morphologic features (8).
In conclusion, sphenoid dysplasia is one of the features of NF-1, but the absence of a sphenoid wing is very rare. By using MDCT, we were able produce good axial and 3D images of the sphenoid bone and the surrounding area.

 XML Download
XML Download