

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The development of image-guided ablation methods for local tumor control has been one of the major advances in the field of oncology (1-3). Many centers have attempted novel approaches for the treatment of a variety of tumors (4-10). The recent publications on this topic have included many articles regarding these new techniques and their therapeutic results. Therefore, it is important to work collaboratively to create a standard nomenclature, usage guidelines, image interpretation criteria, follow-up methodology, and guidelines for reporting therapeutic outcomes in order to facilitate uniform usage and adoption of these technologies before image-guided tumor ablation is used more widely in clinical practice. In 2003, a proposal by the International Working Group on Image-Guided Tumor Ablation was published in Radiology (11). This report on consensus-based recommendations for standardizing terminology for image-guided tumor ablation has been extremely useful in clinical practice and research. The initial report was presented by the Technology Assessment Committee of the Society of Interventional Radiology in 2005 and the updated version of this report was presented in Radiology (2005) and The Journal of Vascular and Interventional Radiology (2005 and 2009) (12-14).
In the field of hepatic surgery, there was a report on the use and dissemination of the Brisbane 2000 nomenclature of liver anatomy and resections, which was adopted by the General Assembly of the International Hepato-Pancreato-Biliary Association at the fourth biennial meeting of that society in Brisbane, Australia in 2000, for evaluating its influence (15). However, there has been no report for determining the incorporation of standardized terminology and reporting criteria for radiofrequency (RF) ablation proposed by the International Working Group on Image-Guided Tumor Ablation in 2003. Therefore, the purpose of the current study was to assess the medical publications on image-guided RF ablation for tumor treatment with respect to the proposed standardized terminology and reporting criteria at 6 years after its inception, with particular focus on procedure terms, imaging findings, therapeutic efficacy, follow-up, and complications.
MATERIALS AND METHODS
Before conducting this study, we developed a detailed protocol for collecting and analyzing data. The main framework for this study was prepared in accordance with guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (16). Formulation and appraisal of the most suitable keywords for searching the PubMed database, such as "neoplasms (Medical Subject Headings [MeSH] term)" and "radiofrequency ablation," were in accordance with evidence-based practice in radiology (17, 18).
Search Strategy and Literature Selection
A systematic search of the medical literature was performed in the following three steps: index keywords, search limited to PubMed, and eligibility criteria. First, a retrospective PubMed search of the world literature from January 2004 to December 2009 was carried out using index keywords. Keyword search using MeSH and free text was performed in combination with the Boolean operator with "neoplasms (MeSH)" and "radiofrequency ablation". Next, we limited searches to human studies and publications in English. Finally, we identified articles according to the following eligibility criteria: 1) original studies, 2) single energy source, 3) non-technical or pathologic reports, 4) reports on non-prostate and dermatologic tumors, Barrett's esophagus, and tumors in the airway, 5) explicit use of terminology for procedure terms, imaging findings, therapeutic efficacy, follow-up, and complications. As stated above, we excluded the reports on prostate and dermatologic tumors, high-grade dysplasia in Barrett's esophagus, and tumors in the airway because the clinical follow-up of prostate tumors after image-guided tumor ablation usually depends on the biochemical status (serum prostate-specific antigen level) and repeat core biopsies rather than imaging modality such as magnetic resonance imaging (19). The decision to perform ablation for Barrett's esophagus and tumors in the airway is based on endoscopic or bronchoscopic surveillance (20, 21), and imaging of dermatologic tumors is generally not performed before initiating the treatment and during the follow-up. The explicit use of terminology in each article was evaluated with respect to the proposed criteria.
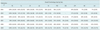
The initial search using the first step yielded 2191 articles. After limiting the PubMed search to only human studies published in English, 1777 articles were identified. Next, we used the titles and abstracts of the identified articles to assess their eligibility. Final selection was then made after reviewing full-text articles (n = 511) that either met the eligibility criteria or regarding which there was any uncertainty with respect to their selection based on the title and abstract. Of these 511 articles, 203 articles were excluded for the following reasons: reporting of only clinical findings (in particular, survival rate) (n = 66), case reports with a variety of forms (n = 54), description of only the imaging analysis (n = 38), technical reports (n = 22), editor notes and letters (n = 12), pathologic reports (n = 8), and others (n = 3). A total of 308 articles were included in the study after the final selection (Fig. 1). Table 1 provides the detailed description of the journals containing articles relevant to this study. In addition, all of the articles relevant to this study are listed in the appendix.
Data Extraction
The entire content of each identified article was reviewed by two radiologists for assessing the use of proposed standardized terminology and reporting criteria using a standard data extraction form, with a focus on the terminology used for procedure terms, imaging findings, therapeutic efficacy and complications. They fully understood the proposed criteria before performing data extraction. The data extraction form consisted of the following five sections according to the classification scheme of the proposed standardized terminology and reporting criteria: 1) baseline study characteristics, 2) terminology for procedure terms, 3) imaging findings, 4) therapeutic efficacy and follow-up, and 5) terminology for complications.
Baseline Characteristics of Articles
The collected data included the following: journal name, year of publication, association with radiology, assessment of accuracy of each term according to the standard terminology, and the use of alternative terms instead of the standard terminology.
Standard Terminology
In this study, assessment of accuracy of the terminology was performed on the basis of the definitions first proposed by the International Working Group on Image-Guided Tumor Ablation in 2003 (11). For assessing the accuracy of the terminology used for procedure terms, the term 'procedure' is preferred rather than the term 'operation', as the latter term implies open surgery. The term 'session' is considered to be synonymous with the term 'procedure'. The term 'procedure' or 'session' refers to a single intervention episode that consists of one or more ablations performed on one or more tumors. In addition, the number of 'procedures' or 'sessions' needed has to be clearly stated. The definition of treatment refers to one or more procedures or sessions.
Regarding the terms used for imaging findings, the term 'index tumor' is used to describe the initially identified tumor before ablation. An 'index tumor' is not referred to as a 'lesion' because it could be confused with the induced coagulation zone or the ablation lesion at imaging. In the same way, the term 'ablation zone' is used after ablation of targeted index tumor is performed to avoid potential confusion because the term 'lesion' is used to refer to both the ablation zone as well as the underlying tumor to be ablated.
For therapeutic efficacy and follow-up, the term 'technical success' is used when a tumor was treated according to the protocol and complete tumor coverage was achieved. Tumor coverage could be assessed either during the procedure or immediately after the procedure. The primary technique effectiveness rate is assessed at a prospectively defined time point (i.e., immediately after the last course of a defined ablation protocol or one week or one month after treatment) when 'complete ablation' of a macroscopic tumor is achieved, as demonstrated by imaging during the follow-up. Therefore, the terms 'technical success' and 'technique effectiveness' must be distinguished from each other. The term 'secondary technique effectiveness rate' includes tumor that have undergone successful repeat ablation after identification of local tumor progression. Local tumor progression is defined as the appearance at follow-up of foci of untreated disease in tumors that were previously considered to be completely ablated.
For assessing the accuracy of terminology used for complications, major complications are defined as events associated with substantial morbidity and disability, an increase in the level of care, hospital admission, or a substantially lengthened hospital stay; all other complications are considered as minor complications. With respect to the above-mentioned terminologies, there were no significant changes in the definitions between 2003 and 2009 (11-14).
Data Analysis
The data from standard data extraction forms were entered into an Excel spreadsheet (Microsoft, Redmond, WA, USA) to facilitate analysis. For evaluation of the accuracy of the terminology used, standard reference terminology was defined according to the guidelines published in 2003 by the International Working Group on Image-Guided Tumor Ablation (11). If a term was used inappropriately throughout the subject articles, it was regarded as incorrect usage. A correct concept means that the definition of the terminology meets the reference standard for the proposed criteria. A correct term means that the term meets the standardized terminology and reporting criteria. Based on these assumptions, we calculated the accuracy of the terminology and alternative terms using a contingency table with the columns 'a' and 'c' (Table 2). We described the results by referring to these two columns as accuracy and alternative terms. Common alternative terms were analyzed according to the frequency of their use. In addition, chronological changes in the frequency of accurately used terms and terminology were assessed in articles published between 2003 and 2009. After this, we evaluated the differences in the accuracy of the terminology according to the medical specialty, the type of radiology journal, and specific journals. Because the reporting standards were published in Radiology and the Journal of Vascular and Interventional Radiology, we compared the compliance with standardized terminology and reporting criteria for RF tumor ablation between the articles published in these two journals and the articles in other radiology journals or other journals that have not implicitly endorsed the reporting standards. For evaluating the trend analysis of compliance with terminology, we defined the new criteria. Tendency towards an increase is defined as an at least 20% increase in the accuracy of each terminology at a research endpoint compared to the baseline accuracy in 2004. In the same manner, stable trend of accuracy means that it cannot achieve more than 20% increment. The Fisher's exact test was used to assess the differences in accuracy, and p-values < 0.05 were considered statistically significant. All of the statistical analyses were conducted with SPSS 17.0 software (SPSS Inc., Chicago, IL, USA).
RESULTS
Identification and Characteristics of Articles
Of the 308 articles (from 81 different types of journals), which met all eligibility criteria and were included in the analysis, the target location for tumor treatment was the liver (n = 184), lungs (n = 38), kidneys (n = 34), bone (n = 22), breast (n = 10), thyroid (n = 5), adrenal gland (n = 5) and others (n = 10). Twenty-nine articles were published in 2004, 38 articles in 2005, 49 articles in 2006, 60 articles in 2007, 62 articles in 2008, and 70 articles in 2009. The other baseline demographic data are described in Table 3.
Accuracy of Terminology and Commonly Used Alternative Terms
Accuracy of the Terms 'Procedure' or 'Session' and 'Treatment'
The accuracy of the term 'procedure' or 'session' was 97% (298/307). Of the 308 articles, 307 articles adopted the correct concept of the term 'procedure' or 'session' according to the proposed reporting criteria. Among these 307 articles, 298 articles used the accurate term, 'procedure' or 'session'. The remaining nine articles used alternative terms. The most commonly used alternative term was 'treatment' (n = 7), followed by 'ablation' (n = 2). With regard to the accuracy of the term 'treatment', among the 308 articles, 300 articles adopted the correct concept of the term 'treatment' according to the proposed criteria. Among these 300 articles, 291 articles used the accurate term 'treatment' with an accuracy of 97% (291/300). The most commonly used alternative term was 'session' (n = 8), followed by 'procedure' (n = 1). One hundred seventy-six of 308 articles clearly stated the number of 'procedures' or 'sessions' needed in the study.
Index Tumor
The accuracy of the term 'index tumor' was 8% (25/307). The accuracy of this term was the lowest among that of the ten terms. Of the 308 articles, 307 articles adopted the correct concept of the term 'index tumor' according to the proposed reporting criteria. Among these 307 articles, only 25 articles used the accurate term 'index tumor'. The other 282 articles used alternative terms. The most commonly used alternative term was 'tumor' (n = 163). The other most commonly used alternative terms were as follows: 'tumor' mixed with 'lesion' (n = 57), 'lesion' (n = 55), 'target or targeted lesion' (n = 6), and 'tumor lesion' (n = 1).
Ablation Zone
The accuracy of the term 'ablation zone' was 65% (103/159). Of the 308 articles, 159 articles adopted the correct concept of the term 'ablation zone' according to the proposed criteria. Among these 159 articles, the term 'ablation zone' was used accurately in 103 articles. The other 56 articles used incorrect alternative terms. The other incorrectly used alternative terms were as follows: 'ablated lesion' (n = 21), 'treated lesion' (n = 9), 'lesion' (n = 6), 'non-enhancing area' (n = 3), 'coagulation zone' (n = 2), 'RFA zone' (n = 2), 'thermal lesion' (n = 2), and 'others' (n = 11).
Technical Success
The accuracy of the term 'technical success' was 55% (52/94). Of the 308 articles, 94 articles adopted the correct concept of the term 'technical success' according to the proposed reporting criteria. Among these 94 articles, 52 articles used the accurate term 'technical success'. The remaining 42 articles used alternative terms to represent the concept of the term 'technical success'. The most commonly used alternative term was 'complete (tumor) ablation' (n = 25). The other most commonly used alternative terms were as follows: 'complete necrosis' (n = 4), 'ablation success' (n = 3), and others (n = 10).
Primary Technique Effectiveness Rate and Secondary Technique Effectiveness Rate
The accuracy of the terms 'primary technique effectiveness rate' and 'secondary technique effectiveness rate' was 33% (42/129) and 94% (17/18), respectively. One hundred twenty-nine of 308 articles adopted the correct concept of the term 'primary technique effectiveness rate'. Among these 129 articles, the term 'primary technique effectiveness rate' was used accurately in 42 articles. The remaining 87 articles used incorrect alternative terms. The most commonly used incorrect alternative terms were 'complete response' (n = 25) and 'complete (tumor) ablation' (n = 25). The other most commonly used incorrect alternative terms were as follows: 'complete tumor necrosis' (n = 16), 'technical success' (n = 5), 'successful treatment' (n = 4), 'successful ablation' (n = 3), 'local control' (n = 2), and 'others' (n = 7). The term 'secondary technique effectiveness rate' was the least frequently used by researchers in the current study. The concept of the term 'secondary technique effectiveness rate' was adopted correctly in only 18 articles, and this term was used accurately in 17 of these 18 articles. The only alternative term used for 'secondary technique effectiveness rate' was 'primary technique effectiveness rate'.
Local Tumor Progression
The accuracy of the term 'local tumor progression' was 45% (88/195). One hundred ninety-five out of 308 articles adopted the concept of the term 'local tumor progression' correctly. Among these 195 articles, 88 articles used the term, 'local tumor progression' accurately. This was the most frequently used term among the terms for 'therapeutic efficacy' and 'follow-up' in the present study. The remaining 107 articles used alternative terms. The most commonly used alternative term was 'local (tumor) recurrence' (n = 63). The other most commonly used alternative term were '(tumor) recurrence' (n = 35), 'intrahepatic recurrence' (n = 2), and 'others' (n = 7).
Major Complication and Minor Complication
The accuracy of the terms 'major complication' and 'minor complication' was 99% (79/80) and 100% (77/77), respectively. Most of the articles used accurate terms instead of alternative terms for complications. The only incorrectly used alternative term for 'major complication' was 'severe complication' (Table 4).
Overall Trend for Usage of Terminology Over the Years
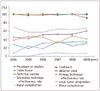
Most of the terminologies used in articles maintained a continuing stable trend over the years. However, the terms 'major complication' and 'minor complication' showed an increasing trend from 2004 to 2009, from 7% to 31% and from 7% to 30%, respectively. Although there was a minimal increase in the frequency of usage of the term 'secondary technique effectiveness rate' during the study period, its overall use was less than 10% (Table 5, Fig. 2).
Overall Accuracy of Terminology Over the Years
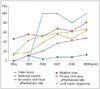
Unlike the stable tendency for usage of all terms over the years, the overall accuracy of terminology was increased every year after the publication of standardized terminology and reporting criteria for image-guided tumor ablation (2003) by the International Working Group, with the exception of the terms 'procedure' or 'session', 'treatment', 'minor complication' and 'major complication'. In addition, the number of published articles increased over time. The accuracy of the term 'secondary technique effectiveness rate' reduced to less than 80% in 2008, whereas the accuracy of the terms 'procedure or session', 'treatment', 'major complication' and 'minor complication' was maintained (at or around 100%) from 2004 to 2009 (Table 6, Fig. 3).
Subgroup Analysis
For the subgroup analysis, we used the total accuracy of each term to calculate the overall accuracy and then compared the overall accuracy between subgroups. Among the ten terms, data of the following four terms 'ablation zone', 'technical success', 'primary technique effectiveness rate', and 'local tumor progression' were included to avoid biased results due to the following confounding factors: 'index tumor' (extremely low accuracy), 'secondary technique effectiveness rate' (used at a very low frequency in the current study), 'procedure or session', 'treatment', 'major complication' and 'minor complication' (almost 100% accuracy in the current study).
Comparison of the Accuracy of Terminology in Articles According to the Medical Specialty
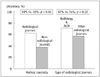
Among the 308 articles, 168 articles were published in radiology journals and 140 articles were published in non-radiology journals. The overall accuracy of terms was significantly greater in the articles published in radiology journals than in the articles published in non-radiology journals (59% vs. 35%, p = 0.01) (Fig. 4).
Comparison of the Accuracy of Terminology in Articles Published in Radiology Journals
Among the 168 articles published in radiology journals, 60 articles were published in Radiology and The Journal of Vascular and Interventional Radiology and 108 articles were published in other radiology journals. The overall accuracy of terms was slightly greater in the articles published in Radiology and The Journal of Vascular and Interventional Radiology than in the articles published in other radiology journals with a statistical significance (67% vs. 54%, p = 0.02) (Fig. 4).
Annual Trend for Accuracy of Terminology in Articles Published in Specific Journals
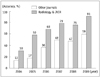
The annual trend analysis for accuracy of terminology in articles published in Radiology and The Journal of Vascular and Interventional Radiology and in those published in other journals showed that there was a continuous increase in the accuracy of investigated terms in the articles published in both categories of journals, from 30% in 2004 to 91% in 2009, and from 13% in 2004 to 59% in 2009, respectively (Fig. 5).
DISCUSSION
The International Working Group on Image-guided Tumor Ablation initiated a global initiative addressing the standardization of terminology and reporting criteria for image-guided tumor ablation in 2001. The major goals of the proposed terminology guidelines were to facilitate uniform comparisons between treatments using either the same or different technologies, to help in effective communication of ideas, and to provide consistency in the terms used to report various aspects of image-guided ablation therapy. After the first version of this proposal was published in 2003, many articles in the field of image-guided tumor ablation have been published in various scientific journals. However, a systematic analysis has not been performed to determine how well the proposed terminology guidelines have been adopted by scientific societies and their associated publications.
In the current study, the term 'index tumor' was the most easily confused term by researchers, with an accuracy of only 8%. Although the term 'index tumor' is preferred for describing the initially identified tumor prior to ablation according to the proposed terminology guidelines, the frequency of the accurate use of the term 'index tumor' has been so low over a relatively long time that an in-depth discussion will be needed to find a solution.
The term 'ablation zone' refers to the area after ablation of the targeted index tumor and it should not to be confused with the term 'lesion' because 'lesion' typically refers to both the ablation zone and the underlying tumor to be ablated. According to our results, accuracy of the use of the term 'ablation zone' improved each year; however, many researchers continue to use alternative terms for the term 'lesion', such as 'ablated lesion', 'treated lesion', 'thermal lesion', and 'lesion' itself.
'Technical success' is an important concept to distinguish patients in whom a given protocol could not be completely executed for either technical reasons or reasons related to co-morbid disease from patients who were treated according to a given protocol. In the current study, the term 'complete (tumor) ablation' was the most commonly used alternative term by researchers to describe technical success. According to the proposed criteria, the correct meaning of the term 'complete ablation' is the opposite to that of the term 'partial ablation'. Therefore, based on this definition, the term, 'partial ablation' should only be used to describe the degree of ablation for index tumors.
We found that the term 'primary technique effectiveness rate' was the second-most inaccurately used term by the researchers. The most commonly used alternative term for the term 'primary technique effectiveness rate' was 'complete response' or 'complete (tumor) ablation'. Complete response is a frequently used parameter for evaluating tumor responses in the field of clinical oncology, and this concept has been supported by guidelines of the World Health Organization criteria (bidimensional perpendicular measurement of tumor size) (22), Response Evaluation Criteria In Solid Tumors (RECIST) (unidimensional measurement of tumor size) (23), and revised RECIST (24). The purpose of using the terms, 'complete response' and 'complete (tumor) ablation' is to describe clinical outcomes following systemic chemotherapy or locoregional therapies according to the measurement of tumor size. The distinction between the terms 'technique effectiveness rate' and 'complete ablation' can be made during the clinical follow-up for determining the effectiveness of the therapy. Thus, these two terms represent different concepts as compared with the term 'primary technique effectiveness rate'.
The term 'secondary technique effectiveness rate' was the least frequently used term among the ten identified terms. The need for a relatively long-term follow-up and difficulty associated with defining the term 'secondary technique effectiveness rate' might have made it difficult to use this term compared to the terms 'technical success', 'primary technique effectiveness rate', and 'local tumor progression', thereby resulting in its infrequent use. Although our study results indicated that the use of this term was associated with a very high accuracy (94%, 17/18), we consider that this result could be due to the bias among a small number of researchers who understand this proposed criteria very well and use this rare terminology to report their therapeutic results. Indeed, among the 17 research teams who used the term 'secondary technique effectiveness rate' accurately, 16 research teams used other terms in their articles with 100% accuracy, with the exception of one team (one research team used the term 'secondary technique effectiveness rate' accurately, but they inaccurately used the term 'complete ablation' instead of the term 'technical success'). Thus, in order to avoid biased results, we excluded this term as well as the terms 'procedure or session', 'treatment', 'minor complication', and 'major complication' from the data set during our subgroup analysis for comparison of the overall accuracy of terminology.
'Local tumor progression' was the most frequently used term for therapeutic efficacy and follow-up, while 'local (tumor) recurrence' was the most commonly used alternative term. Many studies of image-guided tumor ablation have shown that it is impossible to determine whether a viable tumor is untreatable and has continued to grow or if a new tumor is growing at the original site. Therefore, the term 'local tumor progression' is preferred over the term 'local (tumor) recurrence.'
Contrary to the above-described terms for imaging findings, therapeutic efficacy and follow-up, the terms 'procedure or session', 'treatment', 'major complication' and 'minor complication' appeared to be widely accepted with a nearly 100% accuracy. Although the accuracy of the term 'procedure or session' was 97%, only slightly more than 50% (176 of 308 articles) of studies clearly stated the number of "procedures" or "sessions" performed. It is very important to mention the total number of 'procedures' or 'sessions' of each treatment for RF ablation of index tumor because it may be one of the factors that affects the technical success of treatment. The terms 'major complication' and 'minor complication' had the greatest accuracy among all of the terms evaluated in our study. This result can most likely be explained by the fact that these definitions have been adopted from pre-existing standards for therapeutic interventions that are widely used and have been recognized for years by the Society of Interventional Radiology (SIR) and surgical specialties (25, 26).
Following the publication of standardized terminology and reporting criteria for image-guided tumor ablation by the International Working Group in 2003, the overall accuracy of each term showed a general tendency to increase every year, with the exception of the terms 'procedure or session', 'treatment', 'minor complication', and 'major complication'. In addition, the number of citations to two representative articles in the journal Radiology increased from 217 in 2003 (11) to 356 in 2005 (13). These results suggest some success after publication of the initial guidelines for the standardization of terminology. However, unlike the increasing trend for the accuracy of the terminology used, most of the terminologies used in each article maintained a continuing, stable trend over the years. Possible explanations for these results include differences in the primary outcomes reported by the article and use of unrelated terms for indicating primary outcomes, which may have been condensed in each article.
Before planning this study, we expected a greater accuracy of terminology in articles published in Radiology and The Journal of Vascular and Interventional Radiology compared to those published in the other journals because the editors of these two journals are responsible for achieving compliance with the proposed standards. Consistent with our expectations, the articles published in these two radiology journals showed the highest overall accuracy for the terms (67%) compared with the articles published in other radiology journals (54%) and non-radiology journals (35%).
The results of the present study demonstrated that the frequency of using accurate terminology for procedure, imaging findings, therapeutic efficacy, follow-up, and complications varied depending on the specific term. For the image-guided RF ablation of tumors, the terms 'index tumor', 'technical success', 'primary technique effectiveness rate', and 'local tumor progression' were accurately used in less than 55% of the articles reviewed during the study period. In particular, the term 'index tumor' had an accuracy of only 8%, which was very low compared to that of the other terms. Although there is no accepted level of accuracy for using the correct terminology, it is clear from the results of this study that there is scope for improvement with respect to the standardization of terminology.
This is the first systematic review of the proposed guidelines for image-guided tumor ablation. Based on our results, the proposed standards have gained importance among the majority of researchers, especially in the field of radiology. Therefore, radiologists who perform and report these procedures should try to increase the use of standard terminology among different specialties. For this purpose, a multidisciplinary consensus meeting may be required in the near future. Any revised proposal should be published in all of the major journals related to the field of clinical oncology. In addition, we think that efforts taken by the International Working Group and SIR to achieve compliance with proposed standards should be continued. Importantly, consistency while reporting therapeutic outcomes should help to perform a meta-analysis and establish reliable, clinical guidelines for image-guided tumor ablation.
This study has several limitations. First, the number of articles, in which the term 'secondary technique effectiveness rate' was used, were relatively small compared with the number of articles in which the other terms were used, and this may have led to an overestimation of the accuracy of the assessed terminology. Therefore, we excluded this data in the subgroup analysis for the assessment of overall accuracy. Second, to improve the efficiency of data collection, the current study focused on selected terms as well as RF as an energy source in tumor ablation. We chose these specific terms because they were used more frequently than the other terms (e.g., terms used in pathology) due to their association with therapeutic outcomes. In addition, RF ablation is the most frequently used technique for local tumor control compared to the other energy sources. Finally, we limited our dataset to articles published between 2004 and 2009 because of our aim to investigate the trend for the use of standardized terminology and reporting criteria in the field of oncology, and to facilitate the revision of the current guidelines. Importantly, the overall accuracy of the terms used for RF ablation in articles published after 2009 was more than 70%.
In conclusion, the results of our study showed that the standardized terms recommended for reporting image-guided tumor RF ablation are gradually being used in research and clinical practice, especially in the field of radiology. More work is needed for complete standardization of terminology, and the other specialties that utilize image-guided tumor ablation should also be included in this process.





 XML Download
XML Download