

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The success of an imaging-guided core needle breast biopsy depends on the post-biopsy management as well as the performance of the biopsy procedure (1). Any core biopsy procedure may fail to sample a cancer, resulting in a benign, often nonspecific pathologic diagnosis, despite optimization of the technique (2). Although there are methods such as specimen radiography or post-biopsy mammography to confirm lesion retrieval after performing a core biopsy, they often provide incomplete information, especially in lesions visualized by sonography only. Correlation of the pathologic result with the imaging findings after biopsy is found to be useful to validate the biopsy result and to offer subsequent management (2-6).
The purpose of this study is to review derived categories and corresponding management for an imaging-pathology correlation after performing a sonography-guided core needle biopsy and to illustrate the selected images for each category, which will provide guidance in the application of this post-biopsy assessment in practice.
Assessment for Concordance
Before beginning the biopsy procedure, all imaging features of a targeted lesion, mammography, sonography, and MRI, should be carefully reviewed. Moreover, the diagnosis criteria for the finding in question as well as setting the probability of malignancy based on these set criteria should be predetermined (7). When the pathology result is received after biopsy, the radiologist can compare the pathologic diagnosis with the expected result from the imaging finding. Images documented during the biopsy should also be carefully reviewed to verify whether the lesion was accurately targeted with regard to sampling the wrong lesion, suboptimal sampling (i.e., patient movement or insufficient penetration), and procedural complications (i.e., bleeding or hematoma formation) (1, 4, 7). A strong working relationship between the radiologist and pathologist is important for imaging-pathology correlation. The pathologist is critical in assessing and communicating the quantitative and qualitative aspects of the biopsy (1, 4).
Categories of Concordance in Imaging-Pathology Correlation
The imaging and pathologic findings are considered to be concordant when the pathologic result provides an acceptable explanation for the imaging feature and discordant when they do not. After the assessment for concordance has been completed, a management plan can be provided. Parikh and Tickman (4) described five possible outcomes of imaging-pathology correlation and suggested corresponding management for each category.
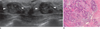
Category 1. Concordant Malignancy
A lesion which showed a suspicious finding for malignancy on images (i.e., Breast Imaging Reporting and Data System [BI-RADS] category 4 or 5) and is diagnosed to be malignant on a subsequent core needle biopsy is a concordant malignancy (4) (Fig. 1). Within this category, appropriate action should be taken without any delay. The radiologist should communicate the biopsy result to the referring physician, and the patient should be informed of the results and referred to a surgeon or oncologist for proper treatment.
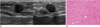
Category 2. Discordant Malignancy
A lesion which typically had benign or benign-favoring imaging features (i.e., BI-RADS category 2 or 3) but proves to be malignant at core needle biopsy falls into this category (Fig. 2). Case management should be identical to that for a concordant malignancy (2, 4). Lesions that usually lie at the circumscribed end of the malignant spectrum can simulate benign nodules; small infiltrating ductal carcinomas, high-grade invasive ductal carcinomas not otherwise specified, metastatic lesions, lymphoma, and special-type tumors that are well circumscribed such as medullary carcinomas, mucinous carcinomas, and papillary carcinoma (8). The radiologist should notify the discordant result to the pathologist and ask the patient to review and confirm the diagnosis. Also, the images of the lesion should be reviewed for image quality, lesion characteristics, and missed associated features which may cause an underestimation of the severity of the lesion. The discrepancy between imaging and pathologic results should be discussed thoroughly.
Category 3. Concordant Benign
A lesion which is initially thought to be benign radiologically (i.e., BI-RADS category 2, 3, or 4a) and also demonstrates benign pathology at core needle biopsy falls into this category (2, 4) (Fig. 3). This result can offer both the physician and the patient reassurance. However, imaging follow-up should be recommended to patients because of delayed false-negative diagnoses at core biopsy (2). Although there is no standard follow-up guideline, a follow-up sonography at six months after biopsy and then annually for at least two years can be recommended (Fig. 4).
Category 4. Discordant Benign
A lesion in this category is suspicious for malignancy at imaging (i.e., BI-RADS category 4 or 5), but demonstrates benign pathologic result after performing a core needle biopsy (2, 4) (Figs. 5-8). Benign lesions with spiculated findings can simulate malignant lesions and be considered as differential diagnoses as follows: sclerosing adenosis, fat necrosis, postsurgical scar, mastitis, granular cell tumor, diabetic mastopathy, and sarcoidosis (8). However, the radiologist should give special attention to discordant benign lesions from which a substantial number of missed cancers at core needle biopsy can be detected without any delay in diagnosis (Figs. 6, 7). In published reports, up to 64% of discordant lesions after a percutaneous biopsy were confirmed as cancer by subsequent surgical excision (5). For a sonography-guided 14-gauge core needle biopsy, discordant lesions had cancer rates of up to 50% (6). If there is concern regarding a discordant benign lesion, it is prudent for the radiologist to immediately contact the interpreting pathologist and thoroughly communicate with each other. According to the discussion, the radiologist should notify the result and discuss the need for a repeat biopsy to the referring physician or the patient. A surgical biopsy, rather than a core needle biopsy, is recommended for a repeat biopsy because of the inconclusive outcome from the first core biopsy. Recently, the vacuum-assisted core needle biopsy has been reported to be an alternative to surgery to obtain a definitive histological diagnosis for discordant benign lesions (9).
Category 5. Borderline or High Risk
A lesion in this category is not malignant but is considered to have an increased lifetime risk for the development of breast cancer (e.g., atypical ductal hyperplasia, lobular neoplasm, radial sclerosing lesion, papillary lesions, possible phyllodes tumors) (2, 4) (Figs. 9, 10). Controversy exists regarding the surgical and oncologic treatment for this lesion. A case-by-case approach is needed to manage the patient in accordance with the active discussion between different subspecialties (4). However, surgical biopsy is usually recommended regardless of concordance, because of the relatively high upgrade rate to malignancy.
BI-RADS Final Assessment Category in Imaging-Pathology Correlation
Since the establishment of BI-RADS for sonography in 2003, the reliability of the sonographic BI-RADS lexicon or classification in evaluating sonographic masses for the likelihood of malignancy have been assessed and reported to have a good performance (10-13). Based on the BI-RADS category, the indication for biopsy of particular lesions can be clarified.
A category 3 lesion is judged to have a 2% or lower probability of malignancy and suggested to be followed up with short-term imaging surveillance. While performing a biopsy is contradictory to a category 3 lesion, it is performed in a specific circumstance such as physician or patient preference. For a category 3 lesion, a benign core biopsy result can be regarded as concordant benign and a malignant core biopsy result as discordant malignant. However, subtle suspicious sonographic features are sometimes overlooked because the final assessment category is determined based on the individual radiologist's experience and training as well as published criteria. In imaging-pathology correlation, therefore, the sonographic features, even for category 3 lesions, should be reviewed based on the strict criteria to avoid missing cancer.
While BI-RADS category 4 lesions have been recommended for biopsy, a wide range of positive predictive value (3% to 94%) is problematic. A new recommendation in the fourth edition of BI-RADS is for category 4 to be subdivided internally into three subgroups (4a, 4b, and 4c) on the basis of the likelihood of malignancy, although optional (14). The BI-RADS did not set out specific guidelines regarding what was the risk of malignancy for each of the subcategories should represent. However, Bent et al. (15) suggested that the guidance range of malignancy likelihood should be 2-10% for category 4a, 11-50% for category 4b, and 51-95% for category 4c. In a study of categorizing lesions by mammography or sonography (11), PPV was 6%, 15%, and 53% for categories 4a, 4b, and 4c, respectively. Whereas, Lee et al. (13) reported that PPV for sonography was 26%, 83%, and 91% for category 4a, 4b, and 4c, respectively. The interobserver variability and poor stratification for the risk of malignancy in the subcategories could be explained by the lack of known factors clearly and objectively defining each subdivision. Because the use of subcategories is optional and clinical data of those subcategories are limited, management is not standardized. Based on BI-RADS (14), the benign core biopsy result may be regarded as concordant benign and the malignant core biopsy result as discordant malignant for a category 4a lesion. The benign core biopsy result may be regarded as discordant benign and the malignant core biopsy result as concordant malignant for a category 4c lesion. For category 4b lesions, close imaging and pathologic correlations are needed. Further studies are needed to evaluate the role of these subdivisions in stratifying the level of suspicion and the use of this information in management decisions.
In conclusions, careful imaging-pathology correlation and appropriated post-biopsy management should be the cornerstone of a successful core biopsy program. It will allow the detection of a substantial number of false-negative results immediately after core needle biopsy by identifying discordant lesions prospectively, thereby avoiding delays in the diagnosis of cancer. Although the communication between the radiologist and pathologist is the basis of imaging-pathology correlation, establishing concordance is subject to the experience of the radiologist. The radiologist performing the biopsy must be familiar with the imaging features of a vast array of pathologic breast lesions and they must be able to correlate with each other.








 XML Download
XML Download