

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Corneal epithelium is crucial for the maintenance of transparency and vision clarity as it provides a smooth refractive surface. Furthermore, corneal epithelial defects must be rapidly restored to avoid further damage to the inner layer. Dry eye syndrome is a common disorder that globally affects 10% to 20% of the adult population [1]. Dry eye is associated with reduced tear aqueous production and abnormalities of the lipid, protein, and mucin profiles. These changes cause desiccation of the ocular surface, leading to epithelial damage as a result of inflammation on the surface. Although dry eye develops from multiple etiologies, it is most often treated with artificial tear supplementation, which promotes epithelial healing [2].
Hyaluronic acid (HA) is naturally occurring glycosaminoglycan of the extracellular matrix that plays an important role in development, would healing, and inflammation [2]. HA has also been used in the treatment of dry eyes because of its long ocular surface residence time and beneficial effect in corneal wound healing by rapid migration of cells leading to prompt wound closure [3].
Recently, a more etiology-oriented approach has been developed by the introduction of diquafosol ophthalmic solution [4]. Diquafosol promotes rather than supplements tear fluid secretion, increases soluble mucin secretion, and upregulates the expression of membrane-associated mucins [5]. Diquafosol is an agonist of purinergic receptor P2Y, G-protein coupled, 2 (P2Y2 receptor), which is a type of nucleotide receptor found on the surfaces of various cells, including epithelial cells and goblet cells in conjunctiva, that play important roles in aqueous and mucin secretion into tear fluid and promotion of tear film stability on the ocular surface [6].
The aim of this study was to compare the cytotoxic and wound healing effects of diquafosol with those of commercially available preservative free topical artificial tear drops (HA) on human corneal epithelium which is easily damaged in dry eye syndrome.
METHODS
Cell lines
This study was performed according to the tenets of the Declaration of Helsinki. The SV-40-transfected human corneal epithelial cell line (HCE-T) was obtained from ATCC (American Type Culture Collection, Manassas, VA), and was grown to 80% confluency in keratinocyte serum-free medium (KSFM) containing 0.05 mg/mL bovine pituitary extract and 5 ng/mL epidermal growth factor in collagen-coated plates. Before treatment, the cells underwent epidermal growth factor starvation overnight, as described [7].
Methyl thiazolyl tetrazolium (MTT) assay
The viabilities of human corneal epithelial cells (HCECs) were determined using a MTT assay. Cells (100 µl; 5×104 cell/mL) were plated in 96-well tissue-culture plates and incubated at 37℃ in 5% CO2 for 24 to 48 h until cultures were subconfluent. Diquafosol (Diquas®, Santen, Osaka, Japan) (100 µl diluted 10%, 20%, or 30%) or 0.3% (Hyaluni®, Taejoon, Seoul, Korea) or 0.18% (Kynex-2®, Alcon, Seoul, Korea) HA were added and incubated for 1, 6, or 24 h. DMEM (100 µl) was added to controls. After 1, 6, and 24 h, plates were washed three times with PBS to remove the drugs. Cell viabilities were evaluated after incubating for 24 h. MTT (3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide; thiazoyl blue, Sigma-Aldrich, St. Louis, MO, USA) (5 mg/mL) was then added to each well. Samples were incubated in the dark for 4 h at 37℃, and media were then removed. Precipitates were resuspended indimethyl sulfoxide (100 µl; DMSO, Sigma-Aldrich). Absorbances were measured on a plate reader at 570 nm. The experiment was performed in triplicate.
Lactate dehydrogenase (LDH) assay
A LDH assay was used to measure leakage of the cytoplasm-located enzyme LDH into extracellular medium. Briefly, HCECs (4.0×103/mL) were seeded into the wells of 96-microtiter plates. Twenty-four hours after seeding, cells were exposed to 10%, 20% or 30% diluted diquafosol, or 0.3% or 0.18% HA, and 1, 6, and 24 h later supernatants were collected. Cell monolayers were then treated with a cell lysis solution for 30 min at room temperature. Cells and lysates were collected and LDH activities were measured in both using the CytoTox96 non-radioactive cytotoxicity assay kit (Promega, WI, USA). Absorbances were measured at 490 nm using a 96-well plate ELISA reader, and LDH activities were expressed as optical densities. Control cells were treated with balanced salt solution. The experiment was repeated three times.
Morphologic assay
HCECs were treated with 3% diquafosol, or 0.3% or 0.18% HA for 24 h and photographed under a phase-contrast microscope. For transmission electron microscopy, cells that had been grown to confluence in 24 well plates were incubated in DMEM containing 3% diquafosol, 0.3% or 0.18% HA, or phosphate buffer (control) for 4 and 8h under 5% CO2 at 37℃. After rinsing with PBS, cells were incubated at 37℃ for 24 h, fixed with 2.5% glutaraldehyde in 0.1 mol/L phosphate buffer (pH 7.4) for 12 h, and postfixed with 0.1% osmium tetroxide for 2 h. After rinsing with 0.1 mol/L of a phosphate buffer and dehydrating in a graded ethanol series, specimens were embedded in an Epon 812 mixture. Ultrathin sections (60~80 nm) were then stained with uranyl acetate and lead citrate, and examined by transmission electron microscopy (JEOL1200EX: Jeol Ltd., Tokyo, Japan).
Scratch wound healing assay
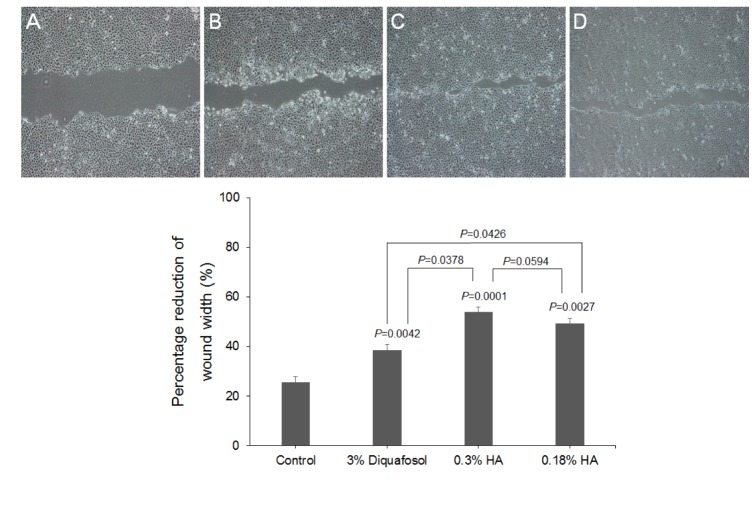
A scratch-wound assay was used to compare the effects of 3% diquafosol and 0.3% and 0.18% HA on corneal epithelial wound healing. HCECs were cultured to confluent monolayers on eight-well chamber slides coated with collagen I (10 µg/cm2; Auspep, Parkville, VIC, Australia) and then scratched with a 100 µl pipette tip. Cells were washed with fresh medium to remove detached cells and incubated in medium in the absence or presence of diquafosol or HA for 24 h. To ensure that the wounds of similar areas were compared, multiple positioning marks were made at the center of denuded surfaces with a needle, and mean distances between wound edges were measured. Twenty-four hours after wounding, monolayers were fixed, and wound areas in marked fields of view were imaged. Mean distances between original and migrated wound edges of three separate samples per treatment were determined using an image analysis system (Image J 1.33o; available by ftp at zippy.nimh.nih.gov/ or at http://rsb.info.nih.gov/nih-imageJ; developed by Wayne Rasband, National Institute of Health, Bethesda, MD, USA), and percentage wound closures in response to diquafosol and HA were compared.
RESULTS
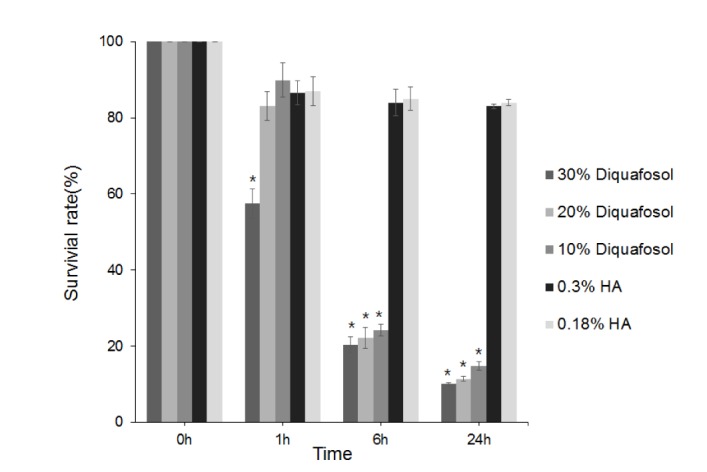
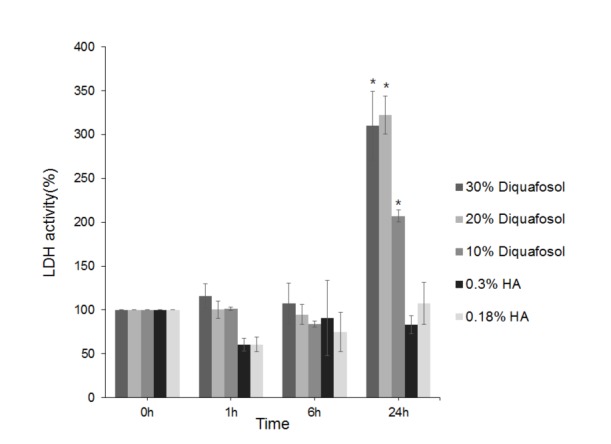
HCEC viabilities after exposure to drugs at different dilutions and for different exposure times are provided in Fig. 1. Cell viability significantly decreased after treatment with 30% diluted diquafosol for 1 hour and 6 hours after treatment with 10% and 20% diluted diquafosol. In contrast, the two HAs did not show any significant cytotoxic effect on HCECs. LDH activities in diquafosol were greater at all exposure times than those of HA, and were significantly greater after 24 hours of treatment (Fig. 2).
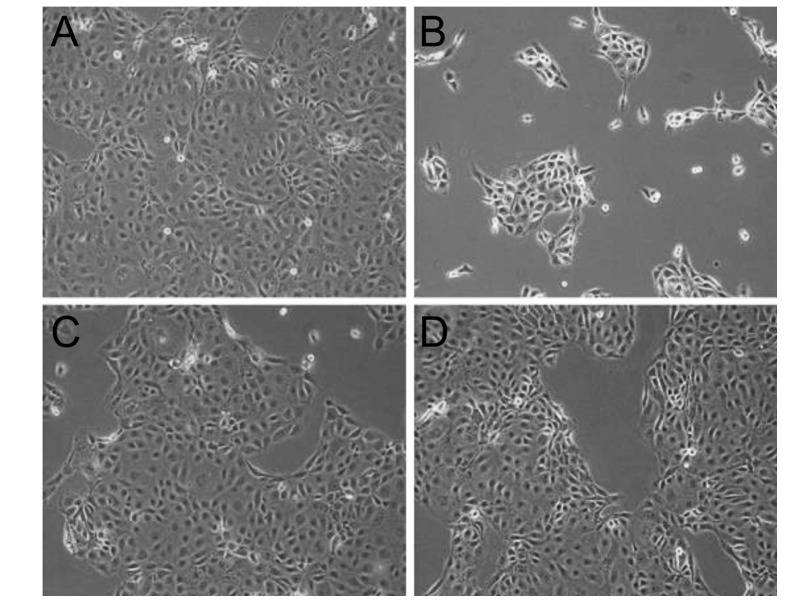
Using phase-contrast microscopy revealed many epithelial cells in control culture media (Fig. 3A), but HCECs were progressively detached from dishes after exposure to 3% diquafosol, or 0.3% or 0.18% HA (Fig. 3B~D) and this detachment was obviously greater for diquafosol (Fig. 3B).
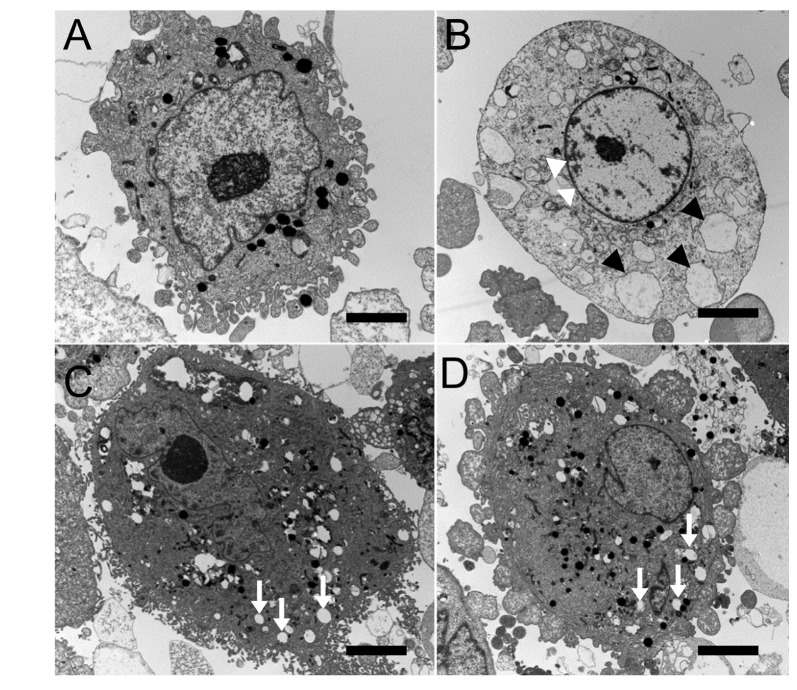
Electron microscopy showed that cells treated with 0.3% or 0.18% HA demonstrated slightly more cytoplasmic bleb formation (Fig. 4C and D) than controls cells (Fig. 4A). Cells treated with 3% diquafosol showed loss of microvilli, larger cytoplasmic vacuoles, presumably caused by cytoplasmic organelles swelling, than controls and condensation of nuclear chromatin along nuclear peripheries (Fig. 4B).
The concentration of Na+ was higher in 3% diquafosol and lower in 0.18% HA, Cl− was lower in 0.18% HA, and K+ was higher in all solutions than normal range. The pH value of 0.3% HA and the osmolarity of 0.18% HA were lower than normal range (Table 1).
Twenty-four hours after wounding monolayers, 3% diquafosol, and 0.3% and 0.18% HA treated HCECs exhibited significantly more wound healing than the control (Fig. 5).
DISCUSSION
Many authors have described the effects of diquafosol on tear films and the clinical parameters of dry eye syndrome [8], but the cytotoxic effect of diquafosol has not been previously evaluated. In the present study, a MTT assay was used to measure NADPH-dependent cellular oxidoreductase enzyme activity, which reflects mitochondrial activity and cell viability, and the presence of the exclusively cytosolic enzyme, LDH, was used as a surrogate of cell membrane damage, and thus, toxicity. According to our results, duration of exposure and diquafosol concentration significantly reduced cell survival and increased cell lysis. On the other hand, no significant difference was observed in HA groups regardless of exposure time. Cell viability significantly decreased after treatment for 1 hour with 30% diluted diquafosol and after treatment for 6 hours with all diluted diquafosol. After treatment with all diluted diquafosol for 24 hours, cell viability decreased and lysis increased, and significant cellular damage was observed. However, in the 0.18 and 0.3% HA, no cytoplasmic membrane or cytoplasmic damage was observed, with the exception of vacuole formation, as we previously reported [9].
Electrolyte contents, pH values, osmolarities, and viscosities of commercially available topical ocular solutions may induce ocular surface damage when they are used for a long period of time or overdosed [10]. Based on our results, K+ concentrations in the three drugs studied were higher than ideal range, although it should be noted the ideal range for extracellular fluid has been reported to be 4.3 to 4.6 mEq/L [11]. Sodium concentration in 3% diquafosol was higher and 0.3% and 0.18% HA was lower than ideal range (142~152.7 mEq/L), and chloride concentration in 0.3% HA was higher and 3% diquafosol and 0.18% HA was lower than ideal range (104.0~117.4 mEq/L) [11]. Osmolarity imbalance can also damage cells. For example, it has been reported that hypertonic stress induced HCEC shrinkage and apoptosis in cell culture models [12]. Drugs with an osmolar pressure in the ideal range (260~320 mOsm/kg) generally do not damage cells [10], and of those drugs examined in the present study 3% diquafosol and 0.3% HA had osmolarities in this range, whereas the osmolarity of 0.18% HA was lower. The pH values of 3% diquafosol and 0.18% HA were both 7.0, and thus, lay in the ideal range (7.0 to 7.7) [13], but 0.3% HA had a pH of 5.5, which could increase corneal epithelial permeability [12]. However, 0.18 and 0.3% HA did not exhibit any significant cytotoxicity, despite these abnormal values, which implies electrolyte concentration, osmolarity, and pH values above and below ideal range are unlikely to impact cellular function despite the fact that they may damage cellular morphology.
Benzalkonium chloride (BAC) is a preservative commonly used in topical ocular solutions. BAC causes surface-active molecules to bind to cellular epithelium and rapidly intercalate into the bilaminar membrane, and thus, BAC can disrupt the precorneal tear film and damage the ocular surface [14151617]. The BAC concentration range in topical ocular solutions typically ranges between 0.004% and 0.025% [18], that is, up to 25 times higher than its lowest concentration. In addition, since the half-life of BAC in corneal epithelial tissues is 20 hours [19], and BAC can remain in ocular tissues for up to 48 hours after application [20], it can cause damage to the ocular surface when eye drops are used long-term. Recently, it was reported that even at the lowest concentration tested, 0.001%, BAC caused significant loss of cellular metabolic activity, and furthermore, this low was observed at exposure times as short as 1 minute [21]. The most significant difference between the three commercial eye solution formulation examined was the presence of BAC. We found in contrast to preserved diquafosol (BAC 0.002%), unpreserved HA hardly induced any cell toxicity, which probably explains the observed cytotoxicity of 3% diquafosol. These results are consistent with those of previous studies, in which cell viabilities were found to be affected more by anti-allergic drugs containing BAC [1415]. Similarly, BAC-containing drugs used to treat other chronic ocular pathologies, like glaucoma, have been reported to be more cytotoxic than preservative free preparations [1617]. In fact, it has been reported that treatment with BAC alone caused cell viability reductions similar to that observed for BAC-containing preparations [2022]. Accordingly, it was suggested BAC was responsible for the observed cell death. Furthermore, this cytotoxic effect was found to persist for over 24 hours.
It is well known that HA stimulates cell migration. In the present study, 0.3% and 0.18% HA promoted wound closure better than the control, and 3% diquafosol was found to promote wound closure as effectively as HA. Interestingly, we observed this effect at a low concentration (2 mg/ml). Byun et al. reported that the effect of diquafosol on corneal epithelial healing was accelerated at concentrations from 20 to 200 µM, but inhibited at concentrations over 2000 µM [23]. This concentration dependence might be related to BAC concentrations in diluted diquafosol, and that whereas diquafosol promotes corneal epithelial wound healing, BAC at higher concentration inhibits this process. It has been previously reported that higher BAC concentrations in diquafosol exhibit more cytotoxic effects [24].
The most obvious limitation of the present study is its in vitro design. However, although in vitro results do not always reflect in vivo effects, we believe that our findings provide a valuable guide with respect to optimal clinical usage. In particular, corneal epithelial toxicity resulting from long term usage or overdoses should be considered, especially in dry eye patients with punctuate epithelial erosion or keratitis.
In conclusion, the present study shows that the main source of cytotoxicity from diquafosol stems from the presence of preservative, which supports mention in other studies of the cytotoxic effects of BAC in topical ophthalmic medications [172526]. Therefore, we suggest a preservative-free solution be adopted as a developmental target, because it would offer a safer option, particularly for long-term or repeated treatment.

 XML Download
XML Download