

 PDF
PDF ePub
ePub Citation
Citation Print
Print


ABBREVIATIONS
bFGF
basic fibroblast growth factor
DPBS
Dulbecco's phosphate-buffered saline
EGF
epidermal growth factor
EPC
endothelial progenitor cell
EPC-CFA
endothelial progenitor cell colony-forming assay
EPC-CFU
endothelial progenitor cell colony-forming unit
FBS
fetal bovine serum
HCY
homocysteine
MNC
mononuclear cell
PECAM-1
platelet-endothelial cell adhesion molecule-1
SCF
stem cell factor
vWF
von Willebrand factor
INTRODUCTION
Circulating endothelial progenitor cells (EPCs) are used as biological markers for blood vessel function [1]. Changes in the number and function of EPCs may be indicative of increased risk for cardiovascular disease [2,3]. A decrease in the number of EPCs could increase coronary artery disease incidence and coronary artery disease related-mortality [4]. Aging, diabetes mellitus, hypertension, hypercholesterolemia, and chronic kidney disease can have a significant negative effect on the number and function of EPCs [5,6,7,8]. A recent study has reported that the number of EPCs and the capacity to form EPC colonies affect health, since EPCs cluster around ischemic damaged tissues to repair the damage. Circulating EPCs differentiate into two types of EPC colony forming units (EPC-CFUs), large sized EPC (large-EPC)-CFUs and small sized EPC (small-EPC)-CFUs. Small-EPC-CFUs and Large-EPC-CFUs define according to cell morphology as round cells or spindle-shaped cells small-EPCs derived from small-EPC-CFU show more immature features. Functionally, the large-EPCs derived from large-EPC-CFU had higher adhesive capacity and tubular forming capacity but lower proliferative potency than small-EPCs [9].
Regular exercise is known to decrease the prevalence of cardiovascular disease [10]. Recently, several independent groups have shown that exercise affects the number and function of EPCs [11]. It was also shown that exercise could increase the number of EPCs, which may improve the function of peripheral and coronary vessels as well as the angiogenic capacity of endothelial cells through nitric oxide (NO) production [12]. Another study has confirmed that tissue ischemia is partially improved by exercise in patients with peripheral and coronary vascular disease; thus, increasing EPCs through exercise in those patients leads to subischemic conditions [13].
Previous findings were mostly derived from studies using animal models, and/or various subgroups of human subjects (patients, athletes, older and younger individuals etc.) [11,12]. The few studies that have been carried out on "normal" (healthy) people tested the effects of short-term exercise (around 4 hours) on EPCs [14]. Therefore, whether healthy people could increase their EPC numbers through exercise remains unknown. The study presented here was designed to find out whether regular exercise training could help healthy people increase the number of EPC colonies. We particularly focused on homocysteine levels since it has been shown that an increase in homocysteine levels in peripheral and coronary vascular disease correlates with a decrease in EPCs [15,16,17]. Our results reveal a strong correlation between exercise, EPC colonies and homocysteine levels.
METHODS
Study subjects
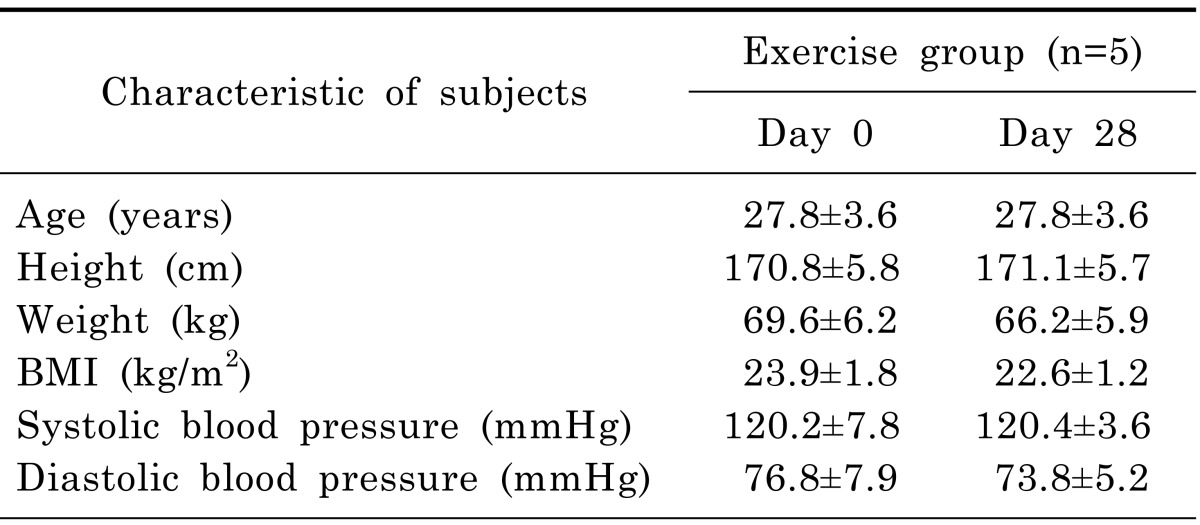
The five healthy volunteers selected for this study were 25~30-year-old disease-free males who had not exercised for 6 months nor consumed alcohol for 2 months prior to the study (Table 1). The volunteers performed a 1-hour long regular exercise every day for 28 days, and their peripheral blood was isolated on days 0 and 28. The Ethics Review Board of the Pusan National University Hospital of Yangsan, Gyeongsangnam-do, Korea, approved the protocols (PNU-2012-19). The experimental study was conducted in accordance with the Declaration of Helsinki.
Exercise training program
The Volunteers performed 30 minutes running on treadmill maintaining 60% of maximum heart rate as aerobic exercise. They did 30 minutes training wet with perspiration including squat, deadlift and bench press as anaerobic exercise. They could start exercise at any time of day.
Isolation of human peripheral blood-derived AC133 positive cells
Human peripheral blood was mixed with Dulbecco's phosphate-buffered saline (DPBS) at a ratio of 1:1, and the mixed sample was then layered on to Ficoll-paque PLUS (GE Healthcare, Sweden) to isolate mononuclear cells (MNCs). After centrifugation, the MNC layer was collected, transferred to tubes, and washed using 2 mM EDTA/PBS. To deplete red blood cells, an RBC lysis solution (Qiagen) was added, followed by gentle mixing and incubation at RT for 10 minutes. To isolate human peripheral blood-derived AC133+ cells with high purity (more than 99%), isolated MNCs were incubated with FcR-blocking reagents and CD133 microbeads, and MACS separation (Miltenyi Biotec) was carried out. Isolated cells were washed with 2% fetal bovine serum (FBS; Gibco) containing MACS buffer.
Colony forming assay
The isolated AC133+ cells were seeded at a density of 1.5×104 cells/35-mm dish in a methyl cellulose-containing medium (H4236; Stem Cell Technologies) supplemented with 20 ng/mL stem cell factor (SCF, Peprotech, Rocky Hill, NJ), 50 ng/mL VEGF (Peprotech), 20 ng/mL interleukin-3 (IL-3, Peprotech), 50 ng/mL basic fibroblast growth factor (bFGF, Peprotech), 50 ng/mL epidermal growth factor (EGF, Peprotech), 2 U/mL heparin (Sigma), 30% FBS, and antibiotics. After 18 days of culture, the colony forming units were identified as large or small colonies by visual inspection with an inverted microscope (Olympus).
Immunofluorescence
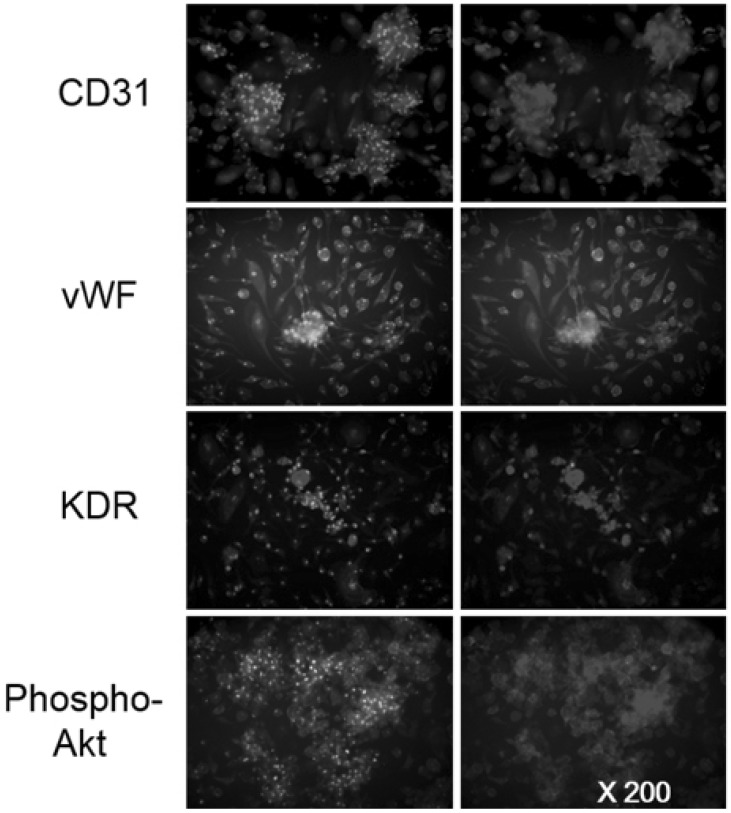
Small and large colony cells were washed with PBS, fixed in 4% paraformaldehyde for 5 min, permeabilized with 0.5% triton X-100 in PBS for 5 min, and incubated at room temperature with PBS containing 3% BSA to block non-specific binding. Colony forming cells were incubated with the following antibodies: goat anti-platelet-endothelial cell adhesion molecule-1 (PECAM-1, CD31) rabbit anti-vWF, anti-KDR (1:100, Santa Cruz), and rabbit anti-phospho-Akt (1:100, Cell Signaling). Cells were incubated overnight at 4℃ with primary antibodies, washed, and then incubated with secondary antibodies (rabbit anti-Alexa 488, goat anti-Alexa 594, and rabbit anti-Alexa594). Images were obtained by confocal microscopy (Olympus, NY).
Plasma homocysteine measurement
Blood was collected during fasting and subsequently centrifuged. Levels of homocysteine were measured using an automated biochemistry analyzer TBA-200FR/NEO (TOSHIBA co., Japan). The conversion concentration of NADH to NAD was measured by a spectrophotometer at 340 nm. Plasma homocysteine was reduced to oxidized homocysteine and combined with serine and cystathionine beta synthase. Normal plasma homocysteine concentrations range from 8.1~17.6 µmol/L in the fasting state in males, and from 5.6~12.9 µmol/L in females.
RESULTS
Characterization of EPC-CFU colony-derived cells
To characterize colony-derived cells after the EPC colony assay using peripheral blood-derived AC133 positive cells, we performed immunophenotyping. Our data showed that colony-derived cells strongly expressed the following endothelial cell lineage surface antigens: CD31, von Willebrand factor (vWF), VEGFR-2 (KDR) and phospho-Akt (Fig. 1) [18].
Regular exercise training tends to increase small as well as large EPC colony formation
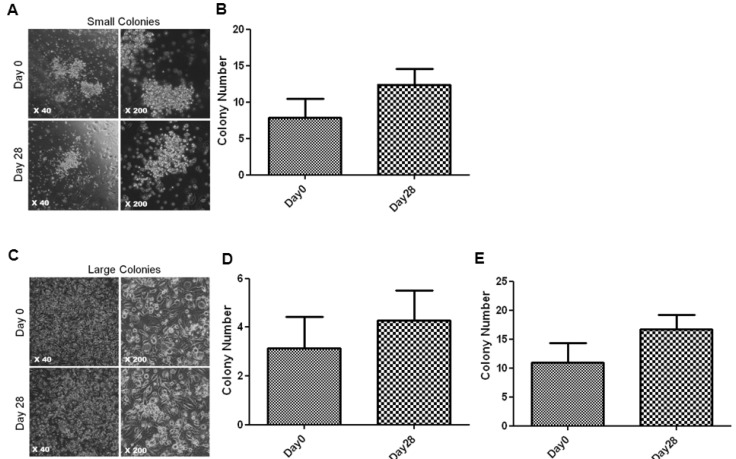
To address whether regular exercise training could help healthy people increase the number of EPC colonies, we assessed the number of small EPCs after a 28-day regular exercise period. We measured the change of small EPC colony number from the peripheral blood of subjects the day before beginning exercise, and the last day of training (Fig. 2A, B). After 28 days of regular exercise training, the number of small-EPC-CFUs was moderately increased and the number of large-EPC-CFUs was increased (Fig. 2C, D). These results show that regular exercise training increases the number of small and large-EPC-CFUs.
Regular exercise training significantly increased total EPC colony formation
We counted the number of total EPC-CFUs to determine the change in the total number of circulating EPCs in the peripheral blood of subjects after regular exercise training. Interestingly, we found that the number of total circulating EPC-CFUs was significantly increased after 28 days of regular exercise (Fig. 2E).
Regular exercise training significantly reduced homocysteine levels
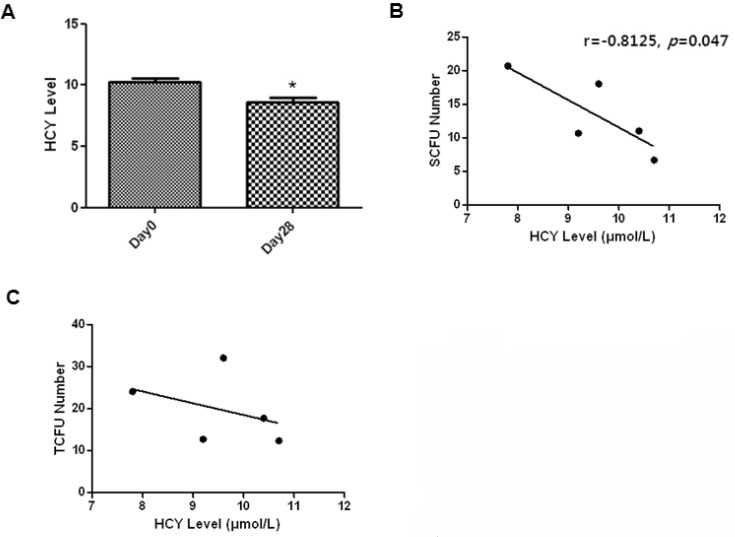
Several lines of evidence suggest that homocysteine affects the number of EPCs by Akt dephosphorylation [15]. To test this hypothesis, we measured the blood levels of homocysteine after regular exercise training. The levels of plasma homocysteine significantly decreased after 28 days of regular exercise training (Fig. 3A). We then asked whether there exists a correlation between homocysteine levels and EPC-CFU. An inverse correlation was observed between small-EPC-CFUs and plasma homocysteine levels in healthy men (Fig. 3B). The small size of EPC-CFU correlates with decreased homocysteine levels (r=-0.8125, p=0.047), suggesting that homocysteine blood levels might influence the type of EPCs formed, which appears as small-EPC-CFUs.
DISCUSSION
Small and large EPCs can be categorized as small-EPC-CFU and large-EPC-CFU respectively. In response to ischemic signals, small-EPCs differentiate into large-EPCs sequentially. However, small-EPCs do not have therapeutic effects due to their low adhesion ability [9]. A previous study reported two types of EPCs-early and late EPCs that contribute to neovasculogenesis equally [19]. The study presented here was designed to determine whether regular exercise training could help healthy people increase their number of EPC colonies. Our main findings are that regular exercise training increases the number of EPC-CFUs in peripheral blood in healthy men, especially the number of total EPC-CFUs. Furthermore, we show that regular exercise training significantly decreases homocysteine levels. Finally, we show that there is an inverse correlation between homocysteine levels and small-EPC-CFU and total EPC-CFU, especially between homocysteine levels and small-EPC-CFU.
It was firstly shown that aerobic exercise training increases the number of EPCs by Laufs et al. [12], and subsequently other studies have reported similar results. A recent study reported a correlation between aerobic exercise training and EPC function. It suggested that the bone marrow, being the main reservoir of EPCs, is influenced by different exercise volume and may be responsible for the improvement of aerobic performance [20]. However, the above mentioned studies were performed on rodents, and it was firstly shown that maximum exercise increases EPCs in human patients with myocardial ischemia by Adams et al. [13]. The subjects in this study however, are not representative of the overall healthy population because they are patients, athletes, or too old/young individuals [11]. Other researchers have used "normal" people in their studies, but they only tested the effect of short-term exercise (just 4 hours) on EPCs [14]. To our knowledge, the study presented here is the first one investigating whether healthy individuals can increase their EPC number through regular exercise. Exercise training increases CFUs, and consequently the function of EPCs [9]. Furthermore, we observed that exercise training increases cd31, vWF, KDR and phospho-Akt that are surface antigens of EPCs [18]. Increasing these antigens through exercise training may improve the function of EPCs.
Previous studies have shown relationships between homocysteine and exercise training [21,22,23]. Zhu and colleagues reported that homocysteine decreases EPC number, function, and activity [15]. Mano and colleagues identified an inverse correlation between homocysteine and EPCs [24]. Taken together, our results and those from previous studies indicate that lower homocysteine levels lead to an increase in EPC number and improves EPC function. High homocysteine levels caused by endothelial injury lead to vascular inflammation, atherosclerosis, and ischemic heart disease. Furthermore, lower homocysteine levels in healthy people is thought to decrease the incidence of coronary disease [25,26]. The number of EPCs also affects cardiovascular condition [27]. Thus, regular exercise training may improve cardiovascular health by increasing EPC-CFU numbers and decreasing homocysteine levels. In this study, we demonstrated that regular exercise training significantly increases the number of EPC-CFU partly by decreasing homocysteine levels in healthy men. The number of EPC-CFUs might thus be a useful a biological marker for exercise training.
This study has its limitations: we did not investigate whether changes in other factors (such as diet) affects the levels of homocysteine or the number of EPCs [24]. Furthermore, the sample size we used is small and it was difficult to study the molecular mechanism of AC133 positive cell-derived EPC sprouting in human peripheral blood samples. Taken together, our results suggest that a 28-day regular exercise program could decrease cardiovascular disease risk in healthy men.
 XML Download
XML Download