

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Retinoblastoma is the most common intraocular malignant tumor in childhood [1]. Although survival rates from retinoblastoma are excellent in industrialized countries, eye salvage and the preservation of vision are still significant challenges. Although radiotherapy is an effective measure for the local control of retinoblastoma, it is considered to be a suboptimal option because it is accompanied by serious complications such as secondary malignancy and orbital deformity. Moreover, cataract formation is the most common ocular complication of external beam radiotherapy in patients with retinoblastoma [2].
Thus, systemic chemotherapy with or without local therapy, such as laser photocoagulation of tumor feeding vessels, cryotherapy, and transpupillary thermotherapy, is now considered to be the first-line globe-conserving therapy in retinoblastoma [23].
Although very rare (incidence less than 1%), the formation of cataracts in eyes affected by retinoblastoma has been well-documented. Radiation therapy is believed to be the major cause of retinoblastoma-related cataracts, but cataracts occur even in patients without a previous history of radiotherapy [4]. There have been a few reports on the prevalence of radiation-induced cataracts in eyes with retinoblastoma and the outcomes of cataract surgery after tumor regression [56789].
However, there has not been a study on secondary cataract formation and the outcomes of cataract surgery following chemotherapy and local therapy, which has replaced radiotherapy as the primary treatment for retinoblastoma. Therefore, the purpose of this study was to assess the visual outcomes, complications, and tumor recurrences in patients at Seoul National University Hospital who have undergone cataract surgery after eye salvage treatment for retinoblastoma.
Materials and Methods
We reviewed the medical records of patients who received eye salvage treatment for retinoblastoma at Seoul National University Children's Hospital between January 1, 1990 and December 31, 2014. The decision for cataract surgery was carefully made after confirmation of tumor regression. Five eyes of five patients underwent cataract surgery.
Complete ocular examinations including keratometry, retinoscopy, fundoscopy, and ultrasound axial length measurements (Otis Instruments, Bryan, TX, USA) were performed preoperatively. For eyes that showed both cataract and macular involvement, we measured the axial length of the contralateral eye to determine the intraocular lens power if the patient had unilateral macular involvement. The postoperative refraction was targeted based on the patient's age at surgery, and the intraocular lens power was calculated using the Sanders-Retzlaff-Kraff II formula. All surgical procedures were performed by the same experienced pediatric ophthalmologist (YSY).
Cataract extraction was performed using bimanual irrigation and an aspiration instrument after mechanical anterior capsulorhexis through scleral tunnel incisions. Posterior capsulotomy and anterior vitrectomy were performed only when there were posterior capsular opacities that obscured the visual axis. After cataract extraction, a foldable, acrylic intraocular lens was inserted into the bag. Sclerotomies and conjunctiva were repaired with 8-0 absorbable suture material. After surgery, the patients were instructed to apply antibiotics drops and topical prednisolone ophthalmic solution for at least 1 month.
The following data were collected: demographic information, age at diagnosis of retinoblastoma, age at the time of surgery, Reese-Ellsworth and international classification of retinoblastoma, interval from retinoblastoma diagnosis to cataract formation, interval from cataract formation to surgery, cataract formation pattern, treatment modalities, the presence or absence of macular involvement, preoperative and postoperative visual acuity, length of follow-up, and intraoperative and postoperative complications. Visual acuity was measured in children using Snellen charts.
Results
Among 464 eyes of 373 patients, 208 eyes (147 patients) received globe-preserving treatment and 17 eyes out of 14 patients developed secondary cataracts during the follow-up periods. The incidence of secondary cataracts was 8.2% in this study period. Nine eyes were treated with both radiotherapy and systemic chemotherapy, and eight eyes were treated with systemic chemotherapy alone.
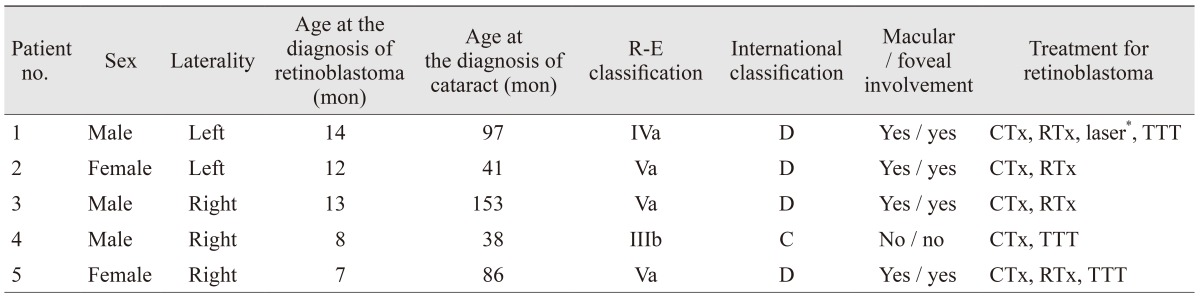
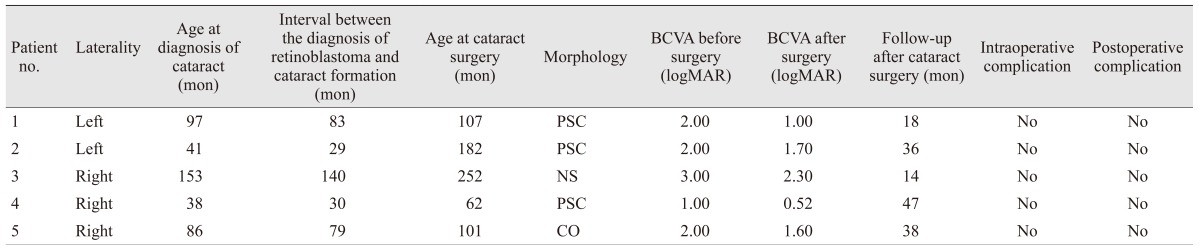
Five eyes (five patients) finally underwent cataract surgery after a safety window. The patient demographics and relevant clinical information of the five eyes are summarized in Table 1.
The median age at retinoblastoma diagnosis was 12 months (range, 7 to 14 months) and the median age of cataract diagnosis was 86 months (range, 38.4 to 153.6 months). Four eyes showed foveal involvement at the initial diagnosis of retinoblastoma and one eye did not have macular involvement. All five patients underwent systemic chemotherapy and radiotherapy was performed in four eyes (radiotherapy was not performed in patient 4). Local treatments such as laser therapy and transpupillary thermotherapy were performed in three eyes (patients 1, 4, and 5).
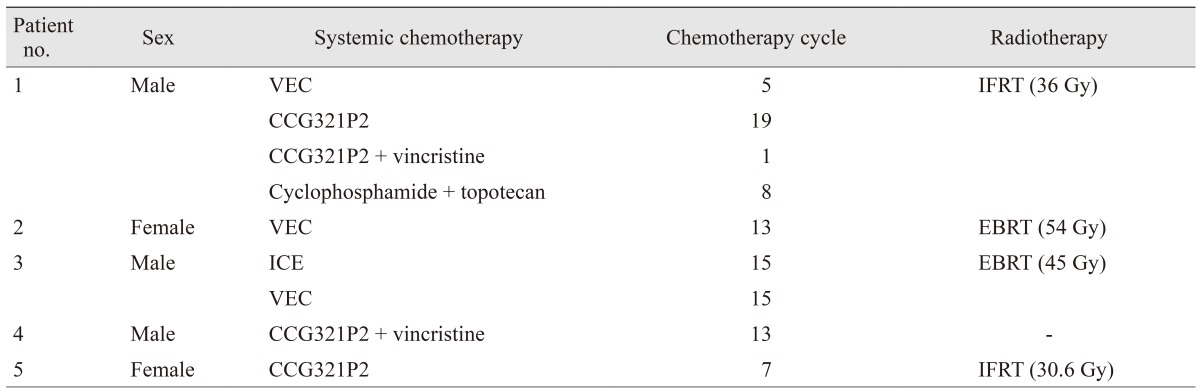
Details of the chemotherapy and radiotherapy treatment are summarized in Table 2. For radiotherapy, patients 1 and 5 received involved-field radiation therapy and patients 2 and 3 received external beam radiotherapy. The absorbed radiation doses were identified. The systemic chemotherapy regimens are shown in Table 2. All patients received different chemotherapy regimens, and patients 1 and 3 underwent a change in their regimens due to tumor progression with the initial chemotherapy choice.
Table 3 describes the characteristics and outcomes of cataract extraction and intraocular lens implantation. The median age at cataract surgery was 8.4 years (range, 5.2 to 21 years). The median interval from retinoblastoma diagnosis to cataract formation was 6.6 years (range, 2.4 to 11.7 years). The median safety window, which is considered to be the interval between the confirmation date of tumor regression and the date of cataract surgery, was 4.1 years (range, 2.3 to 11.4 years). The morphology of the cataract varied among the five patients. Posterior subcapsular cataracts were identified in patients 1, 2, and 4; a nuclear sclerotic cataract was identified in patient 3; a cortical cataract was identified in patient 5.
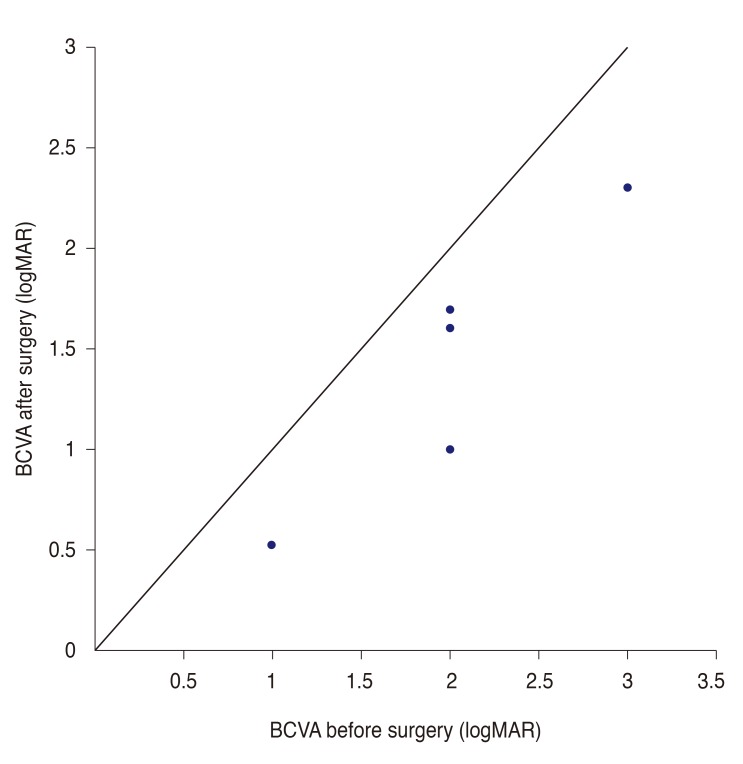
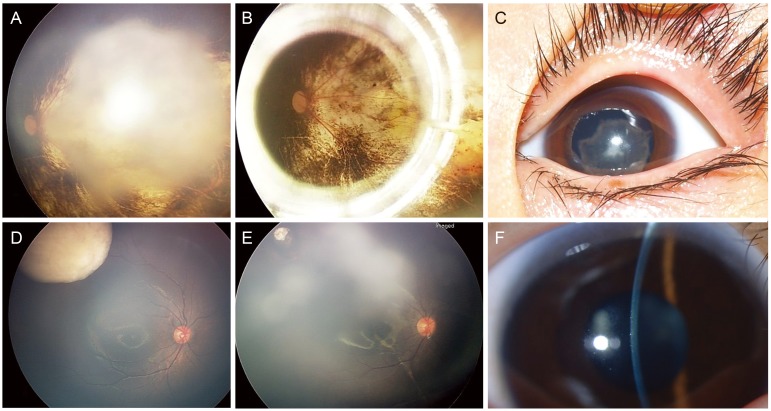
The median follow-up period after cataract surgery was 36 months (range, 14 to 47 months). The mean preoperative visual acuity was logarithm of the minimum angle of resolution (logMAR) 2.00 (range, 1.00 to 3.00) and the mean postoperative visual acuity improved to logMAR 1.42 (range, 0.52 to 2.30). All patients reported better visual acuity after cataract surgery (Fig. 1). In eyes without foveal involvement, a fair final vision was achieved. The representative fundus photographs and anterior segment photos are shown in Fig. 2A-2F. No intraoperative or postoperative complications were encountered. For patient 4, the posterior capsule was left intact at the time of surgery, and the patient subsequently required a neodymium-yttrium aluminum garnet (Nd:YAG) laser capsulotomy. After laser capsulotomy, no immediate or long-term complications were detected during the 47 months of the follow-up period. No intraocular recurrence, extraocular extension, or metastasis was noted at the final follow-up examination in any of the patients.
Discussion
We report a series of five retinoblastoma patients who underwent surgery for secondary cataracts that developed after eye salvage treatment (radiotherapy, systemic chemotherapy, and local therapy). Cataract extraction after regression of the retinoblastoma was not associated with retinoblastoma recurrence or metastasis after a median follow-up period of 36 months. Of the five patients, all five eyes showed improved visual acuity after cataract surgery, even in the presence of foveal involvement.
Intraocular surgery after the treatment for retinoblastoma poses unique challenges because of the risk of the dissemination of tumor cells at the time of surgery. Brooks et al. [6] reported three cases of tumor recurrence. Honavar et al. [10] reported five cases of recurrence, and Moshfeghi et al. [11] reported one case of retinoblastoma recurrence after cataract surgery. In our cases, there was no evidence of retinoblastoma recurrence and metastasis. Predisposing factors such as vitreous seeding and anterior tumors are known to be risk factors for tumor recurrence and were not observed at the time of surgery [8]. The median safety window was 4.1 years in our case series, which is considered to be a safe time window for intraocular surgery according to previous studies suggesting that the quiescent interval be at least 16 months to prevent tumor recurrences [5812].
We performed cataract surgery via a superior scleral tunnel incision. Clear corneal and pars plana approaches have been used with success in children undergoing cataract surgery, with no evidence of tumor recurrence [61213]. However, we prefer a scleral tunnel approach because it results in a more secure wound and reduces postoperative complications such as wound leaks.
Posterior capsule management in pediatric cataract surgery is important in eyes previously treated for retinoblastoma because the posterior capsule is believed to be a barrier to tumor spread [1415]. However, primary posterior capsulotomy and anterior vitrectomy are frequently performed to avoid the risk of cataract development, even in eyes with a prior history of retinoblastoma. In this series, two eyes that underwent simultaneous posterior capsulotomy and anterior vitrectomy during cataract extraction and one eye that received Nd:YAG laser capsulotomy for a cataract did not show any postoperative tumor-related complications. Therefore, it is necessary to consider performing posterior capsulotomy and anterior vitrectomy based on individual patient characteristics as well as the characteristics of the retinoblastoma and cataract.
In this case series, we reviewed five patients and five eyes that underwent cataract surgery after retinoblastoma treatment. Previous studies have mostly focused on radiation-induced cataracts and the visual outcomes after cataract extraction [678910121415]. In our study of retinoblastoma patients, a 4.5% incidence rate of radiation-induced cataract formation was observed with 30 to 54 Gy irradiation, which is higher than the 1% to 2% incidence rate of cataract due to radiation toxicity from head and neck cancer treatment with 54 to 60 Gy irradiation reported in the previous literature [16]. In our study, four eyes received both radiotherapy and chemotherapy, and one eye received only systemic chemotherapy and local therapy. Among the 12 eyes that did not undergo cataract surgery, seven eyes were treated with systemic chemotherapy alone, while the other five eyes were treated with both radiation and chemotherapy. Given the preference of using systemic chemotherapy for eye salvaging treatments [1718], the incidence of chemotherapy-induced cataracts needs to be addressed. We hypothesize that systemic chemotherapy can trigger the formation of secondary cataracts.
In conclusion, cataract surgery in patients with secondary cataract formation after retinoblastoma regression is a safe way to improve visual acuity and quality of life, even if the tumor lesion involves the macular and foveal area. We recommend cataract surgery in retinoblastoma patients after a proper safety window is achieved. Further investigations are needed to elucidate the pathogenesis of the chemotherapy-induced secondary cataracts.
 XML Download
XML Download