

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Macular edema is the main cause of visual impairment in diabetic patients.1 The Early Treatment Diabetic Retinopathy Study trial showed that focal laser photocoagulation is beneficial for eyes with clinically significant diabetic macular edema.2 However, the therapeutic value of scattered laser coagulation of the macula when capillary leakage and macular edema diffusely involve the posterior pole of the fundus has not been conclusively shown.3
Recent investigations have reported the use of intravitreal triamcinolone acetonide (TA) for treatment of diffuse diabetic macular edema.4,5 The exact mechanism of effects is not known, but triamcinolone is presumed to diminish retinal leakage and reduce retinal thickening in the macula, leading to improved visual acuity.6
Different doses varying from about 4 mg to about 20 mg TA have been employed thus far. Whether efficacy and duration of the effect of intravitreal TA are dosage-dependent is unknown. Spandau et al.7 reported that the efficacy of intravitreal TA was dosage-dependent, and treatment response lasted longer, and was more pronounced with increasing dosage.
The purpose of this study was to investigate the dosage-dependency of the duration and efficacy of intravitreal TA in the treatment of diffuse diabetic macular edema.
Materials and Methods
This clinical retrospective study included 44 eyes (40 patients) with diabetic macular edema, defined according to the Early Treatment Diabetic Retinopathy Study (ETDRS). All patients were treated randomly with 4 mg, 8 mg, or 25 mg TA intravitreally, from 2004 June to 2005 May.
Assessment of diabetic macular edema was based on ophthalmoscopic examination, fluorescein angiography and OCT of the macula. The patients consisted of 19 men and 21 women with a mean age of 60 years (standard deviation [SD] 10; range 43-83 years). Mean follow-up was 9.8 months (SD 2.3; range 5-12 months). Macular thickness at baseline was 559 µm (SD 228; range 174-1263 µm). LogMAR visual acuity at baseline was 0.77 logMAR units (SD 0.44; range 0.2-2 units). Mean intraocular pressure (IOP) at baseline was 14 mmHg (SD 2.5; range 9-19 mmHg) (Table 1).
Treatment with TA was intravitreal, with 12 eyes (27%) receiving 4 mg, 17 (39%) receiving 8 mg, and 15 (34%) treated with 25 mg. No patients received reinjection. During follow-up, if ocular surgery or other ocular treatment of diabetic retinopathy had been performed, the patients were regarded as dropped at follow-up. All eyes included into the study received their last retinal laser treatment at least one month before inclusion into the study. If the criteria for retinal laser treatment according to the ETDRS study were fulfilled, laser treatment was performed. None of the eyes had received intravitreal injection before inclusion into the study. Randomization of patients into study groups was masked by the hospital pharmacy.
The hospital pharmacy prepared the TA for intraocular injection by extracting 0.1 mL (for an intended dosage of 4 mg) or 0.2 mL (for 8 mg) from a vial (Rheudenolone®, 40 mg/mL Kukje pharmacy, Korea) containing 40 mg of TA in 1 mL. The extracted volume was put into a tuberculin syringe (1 mL). An intended dosage of 25 mg was prepared from 0.1 mL precipitate after erecting the syringe for 1 hour before extracting 1 mL from the vial. Concentrations were measured by High Phase Liquid Chromatography assay.
The extracted TA was injected into the vitreous after instillation of 0.5% propacaine hydrochloride (Alcaine®, Alcon, USA) and 5% povidone iodine. The injection was performed 3.5 mm posterior to the limbus, through the inferior pars plana, with a 30-gauge needle. All patients were given levofloxacine drops (Cravit®, Santen, Japan) as a prophylactic treatment.
Visual acuity, macular thickness, and IOP baselines were determined at the beginning of the study. Macular thickness was measured by optical coherent tomography (OCT 3) (STRATUS-OCT Model 3000, Carl Zeiss Meditec Inc., San-Leandro. CA) and IOP was measured by Goldmann applanation tonometry (GAP). Visual acuity was determined in a standardized fashion by an observer performing best corrected refractometry, with measurements converted into the logarithm of the minimum angle of resolution (logMAR). Macular thickness was determined manually with an OCT 3 measurement by a sophisticated examiner. IOP with GAP was measured by the same doctor. Visual acuity and IOP were re-examined the first day after the injection, then after 1 week and 1, 2, and 3 months after the injection, and then at 3-month intervals. Macular thickness was rechecked at 1, 3, 6, 9, and 12 months. Mean follow-up was 9.8 (SD 2.3) months (range 5-12 months).
Statistical analyses were performed using a commercially available statistical software package (SPSS® for Windows, version 12.0, SPSS, Chicago, IL, USA) for analysis of variance (ANOVA), chi-square test, Wilcoxon signed-rank test and Mann-Whitney test. The post-hoc test was done with Tukey analysis. The level of significance was 0.05 (two-sided) for all statistical testing.
Results
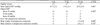
In the first investigation, the 4 mg, 8 mg, and 25 mg study groups contained 12, 17, and 15 eyes, respectively, while in the final investigation, they contained 6, 9 and 6 eyes. Diagnoses, ages, and follow-up periods were not significantly different among the three study groups (p=0.43, 0.51, 0.19), and there were no statistical differences in preoperative macular thickness, visual acuity, or IOP among three groups (p=0.97, 0.49, 0.16) (Table 2).
Macular thickness during follow-up
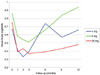
In the 4 mg study group, macular thickness decreased significantly (p=0.002) from 566 µm at baseline to a peak of 218 µm at the 1-month follow-up. The thinnest region of macular thickness increased to a thickness of 653 µm at 12 months after injection. After the 3-month follow-up, macular thickness differed significantly from the baseline value (p=0.005). Macular thickness at baseline (566 µm) and at the 6-month follow-up (513 µm) did not differ significantly (p=0.345). Macular thickness at the 9-month follow-up (737 µm) and the 12-month follow-up (653 µm) was thicker than at baseline (566 µm; p=0.741 for 9-month and p=0.712 for 12-month; Table 3, Fig. 1).
In the 8 mg study group, macular thickness decreased significantly from 565 µm at baseline to a plateau of 213 µm (p=0.001) to 247 µm (p=0.002) at 1 and 3 months after injection. It increased to a value of 656 µm at 12 months after injection. Macular thickness obtained at the 6-month follow-up was significantly thinner than baseline (350 µm; p=0.003). Macular thickness at the 9-month (611 µm) and 12-month (656 µm) follow-ups was thicker than at baseline (565 µm p=0.225 and p=0.295; Table 3, Fig. 1).
In the 25 mg study group, macular thickness decreased significantly from 546 µm at baseline to a plateau between 182 µm (p=0.001) at 1 month after injection, 197 µm (p=0.001) at 3 months after injection and 216 µm (p=0.018) at 6 months after injection. At the 9-month and 12-month follow-ups, macular thicknesses were 309 and 314 µm, which were thinner than baseline (546 µm) but not significantly different (p=0.2650 for 9-months and p=0.114 for 12-months; Table 3, Fig. 1).
Among the three groups, there were significant differences in macular thickness at 6, 9 and 12 months. At 6 months, macular thickness was significantly different (p=0.036), especially between the 4 mg and 25 mg groups (p=0.028). At 9 months, macular thickness was significantly different (p=0.008), especially between the 4 mg and 25 mg group, and also between the 8 mg and 25 mg groups (p=0.009 and 0.029). At 12 months, comparison of macular thickness showed significant differences among the three groups (p=0.002). The macular thickness of the 25 mg study group was significantly thinner than in the other groups at 9 and 12 months (p<0.05; Fig. 1).
Visual acuity during follow-up
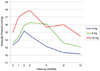
In the 4 mg study group, increase in visual acuity was significantly (p=0.003), from 0.67 logMAR unit at baseline to a peak of 0.39 logMAR unit at the 3-month follow-up. From this peak value, it decreased to 0.66 at 12 months after injection. Visual acuity obtained at 1 week (0.46 logMAR unit), 1 month (0.41 logMAR unit) and 3 months (0.39 logMAR unit) differed significantly from the baseline visual acuity (p=0.005, 0.002, and 0.003). Visual acuity at 6, 9 and 12 months (0.73, 0.57, 0.66 logMAR unit) did not differ significantly from the baseline (0.67 logMAR unit; p=0.594, 0.115, 0.374; Table 4, Fig. 2).
In the 8 mg study group, increase in visual acuity was significant (p=0.001), from 0.86 logMAR unit at baseline to a peak of 0.51 logMAR unit at the 3-month follow-up. From this peak, it decreased to a value of 0.94 logMAR unit at 12 months after injection. Visual acuity obtained at 1 week (0.55 logMAR unit), 1 month (0.57 logMAR unit), 3 months (0.50 logMAR unit), and 6 months (0.66 logMAR unit) differed significantly from the baseline (p=0.001, 0.002, 0.001, and 0.007). Visual acuity at the 9 and 12 month follow-ups (0.88, 0.94 logMAR unit) did not differ significantly from the baseline (p=0.989, 0.414; Table 4, Fig. 2).
In the 25 mg study group, visual acuity increased significantly (p=0.018) from 0.75 logMAR unit at baseline to a peak of 0.37 logMAR unit at the 3-month follow-up. From this peak, it decreased to a value of 0.48 logMAR unit at 12 months after injection. Visual acuity at 1 week (0.54 logMAR unit), 1 month (0.39 logMAR unit), 3 months (0.37 logMAR unit), and 6 months (0.39 logMAR unit) differed significantly from the baseline (p=0.007, 0.005, 0.001, and 0.018). Visual acuity at the 9- and 12- month follow-ups (0.42, 0.48 logMAR unit) did not differ significantly from the baseline (p=0.181, 0.310; Table 4, Fig. 2).
At 9 and 12 months, visual acuity showed significant differences between the three groups (p=0.016, 0.002). At 9 and 12 months, comparisons between the 4 mg and 25 mg group, and also between the 8 mg and 25 mg groups showed significant differences (p<0.05), with the 25 mg group having better visual acuity (Fig. 2).
IOP during follow-up
In the 4 mg study group, IOP increased slightly, from 13.7 mmHg at baseline to a peak of 14.7 mmHg at the 3-month follow-up, however the change was not statistically significant (p=0.232). From the peak value, it decreased to 12.2 mmHg at 12 months after injection. IOP obtained through the follow-up period did not differ significantly from the baseline (Table 5, Fig. 3).
In the 8 mg study group, IOP increased from 13.7 mmHg at baseline to a peak of 15.8 mmHg at the 3-month follow-up and the change was statistically significant (p=0.015). From the peak value, it decreased to 15.4 mmHg at 12 months after injection. IOP measurements obtained through the follow-up period did not differ significantly from the baseline IOP, except at 3 months (Table 5, Fig. 3).
In the 25 mg study group, IOP increased from 15.0 mmHg at baseline to a peak of 19.9 mmHg at the 6-month follow-up, but the change was not statistically significant (p=0.171). From the peak value, it decreased to 14.5 mmHg at 12 months after injection. IOP obtained through the follow-up period did not differ significantly from the baseline (Table 5, Fig. 3).
At 6, 9, and 12 months, significant differences in IOP were seen among the three groups (p=0.027, 0.025, 0.028; Fig. 3). In particular, analysis of the 4 mg and 8 mg groups showed significant differences at 6 and 12 months (p=0.025, 0.027). Analysis of the 4 mg and 25 mg groups showed differences (p=0.025) at 9 months (Fig. 3).
The mean highest intraocular pressures during follow-up were 16.7 mmHg (4 mg study group), 17.8 mmHg (8 mg study group), and 22.8 mmHg (25 mg study group). IOP in the 25 mg study group was significantly higher than that of the other groups (p=0.001). The number of eyes for which the highest IOP measured below 22 mmHg in each group were 12, 15, and 7 respectively (p=0.002). The number of eyes for which the highest IOP ranged from 22 mmHg to 30 mmHg was 2 of 17 in the 8 mg study group, 6 of 15 in the 25 mg study group and none in the 4 mg study group. The number of eyes for which the highest IOP measured above 30 mmHg was 2 of 15 in the 25 mg study group. Antiglaucoma medication was not needed in the 4 mg study group, but required in the 8 and 25 mg study groups. The number of eyes that required antiglaucoma medication was 1 of 17 in the 8 mg study group and 6 of 15 in the 25 mg study group. The mean number receiving antiglaucoma medications was 1 in the 8 mg study group and 1.5 in the 25 mg study group (p=0.6). The mean duration of antiglaucoma medication was 2 months in the 8 mg study group and 2.8 monthsin the 25 mg study group (p=0.533).
Discussion
Recent studies have suggested that intravitreal TA may be useful for increasing visual acuity in patients with diffuse diabetic macular edema.8,9 In previous studies, the effect of intravitreal TA was studied using follow-up periods of up to 6 months. Jonas et al.10 observed a significant improvement in visual acuity up to 6 months after injection of 25 mg TA. Martidis et al.11 injected a lower dose (4 mg) and reported a visual improvement and a reduction in macular thickness of 58% and 38% at 3 and 6 months, respectively. On the other hand, Massin et al.,8 also using 4 mg TA, found no significant beneficial effect on visual acuity, although a significant reduction in macular thickness was observed using OCT, until 3 months. Recently, Jonas et al.10,12 reported favorable results with a higher dose of TA (25 mg).
Using a dosage of about 20 mg, the increase in visual acuity was most marked for the first 3-6 months after the injection, and was present during a period of about 6-9 months.12 At 4 mg, the duration of the effect, as measured by a reduction in macular thickness by optical coherence tomography, was less than 6 months.8,11 At the end of follow-up, visual acuity measurements often returned to baseline values with no significant difference between the final baseline values.8,11 These investigations, which indirectly compare the duration of the effect of intravitreal TA, have been confirmed by the present study.
This study showed that the duration of intravitreal TA effect on macular thickness increased with increasing dosage (Table 3). The 8 mg study group showed effects similar to the 25 mg study group through the 6-month follow-up. Interestingly, in the 25 mg study group, macular thickness at the 9- and 12-month follow-ups (309 µm), was thinner than at baseline (546 µm), although not significantly so. In this period, the 4 mg and 8 mg study groups showed thicker macular thickness than baseline (Table 3, Fig. 1).
The duration of the TA effect on visual acuity increased with increasing dosage (Table 4). The 8 mg study group did not differ from 25 mg study group through the 6-month follow up. Interestingly, visual acuities in both the 4 mg and 25 mg study groups at the 9- and 12-month follow-up were higher but not significantly increased from the baseline visual acuity (Table 4, Fig. 2).
These data may suggest that for at least 6 months, the amount of post-injection increase in visual acuity and the duration of the effect of intravitreal TA show a dosage dependency, which is lost after 6 months. This may have implications for discussions on the dosage of intravitreal TA to be used as treatment for diffuse diabetic macular edema, and on how to reduce the frequency of required intravitreal reinjections. Future studies are necessary to evaluate the optimum dosage with regard to tolerability, side effects, and duration of action.
The main side effect of intravitreal TA observed in the present study was an increase in IOP. Consistent with previous studies,13-15 the secondary ocular hypertension could usually be treated with topical antiglaucoma medication without the development of glaucomatous optic nerve damage. Ten (23%) eyes developed maximal IOP measurements higher than 21 mmHg. The mean highest IOP during follow-up was significantly higher in the 25 mg study group than in both the 4 mg and 8 mg groups (Table 6). This suggests that the possibility of high dosages of intravitreal TA leading to IOP elevation must be taken into account. These results are different from previous independent investigations, in which the frequency of elevated IOP after the intravitreal injection of TA did not vary between studies using a dosage of 4 mg compared with studies using a dosage of about 20 mg.14,16
Other than the side effect of elevated IOP, none of the study groups showed infection, or a marked progression of cataracts as assessed by slitlamp biomicroscopy.17-21 The study sample, however, may have been too small to statistically address these questions, since most side effects such as infectious endophthalmitis, may have a frequency of less than 1%.
A limitation of the study might be that, although intravitreal TA increased the degree of cataracts, cataract surgery was not performed in combination with, or after, the intravitreal injection of TA during follow-up. The vision-reducing effect of progressive cataracts might have hidden some of the vision-improving effects of TA. Another limiting factor of this study might be the relatively small number of patients and the decrease in the number of those patients after the 6-month follow-up. Nonetheless, the postinjection increase in visual acuity, as well as the duration of the effect, were larger in both the 8 mg and 25 mg study group than in the 4 mg study group.
In conclusion, these data suggest that treatment response may last longer with a dose of 8 or 25 mg TA compared to a dose of 4 mg, in patients with diffuse diabetic macular edema. The increase in intraocular pressure induced by TA may not be strictly associated with the dosage used.






 XML Download
XML Download