

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The 2015 cardiopulmonary resuscitation (CPR) guideline recommends that the lone healthcare provider should use the two-finger chest compression technique (TFCC) instead of the two-thumb encircling hands technique (TTHT) when performing CPR on an infant in cardiac arrest (1). However, the guideline does not describe the exact method to be used during TFCC, i.e., which fingers and which hand.
In case of two-handed chest compression technique, the chest compression force is proportional to the rescuer’s upper body mass (2). In TFCC, however, the full mass of the upper body is not loaded onto the compression point. Therefore, the quality of TFCC might be influenced by other factors, such as finger or hand strength.
We hypothesised that the quality of TFCC could be improved by using two fingers of the right hand, because the hand grip power of the right hand is typically greater than that of the left hand regardless of handedness (345) and that TFCC performance would be better with the use of two fingers of similar lengths because the rescuer might not be able to maintain a stable finger posture with two fingers of greatly differing lengths.
MATERIALS AND METHODS
Study design
The study was a prospective randomised cross-over trial. Two cross-over trials based on four different experiments were conducted randomly (Fig. 1). The participants were randomised three times throughout the trials using randomisation lists created by assigning random-number sequences obtained by a web-based program to six permuted blocks with the initial of each group, “A” or “B” (6). Five-minute rests were provided between the tests.

Study setting and population
This study was conducted in the emergency department of a university hospital using a model of infant cardiac arrest in which the “patient” was a 3-month-old-infant-sized manikin (Resusci Baby QCPR, Laerdal Medical, Stavanger, Norway) between June 2015 and July 2015. Healthcare providers who were certified basic-life-support providers participated in the study after providing written informed consent. The exclusion criteria were an inability to perform CPR because of a recent finger or hand injury and refusal to participate in the study. Ultimately, 30 healthcare providers were recruited.
Sample size was calculated based on chest compression depth as the primary outcome variable. The two-sided significance level was set at 0.05, and the power of the test at 80%. The standard deviation of the mean compression depth (MCD) was 5 mm, based on published results (7). The allowable difference in MCD between TFCC with the right vs. left hand was 10% (2.6 mm) of the MCD. The minimum number of participants in each group was calculated using a web program (sample size calculator: two cross-over sample means) and determined to be 15 (8).
Study protocol
The infant manikin was placed on a hard floor in the supine position. The participants performed single-rescuer CPR with 30:2 compression: ventilation using TFCC for 2 minutes. Ventilations were performed using the mouth-to-mouth method and a Manikin Face Shield (Laerdal Medical).
The fingers used in the TFCC were limited to the index-middle fingers and the middle-ring fingers because the thumb and little finger are very different in length. Therefore, the participants performed TFCC with the index-middle fingers of the right hand (Test 1), index-middle fingers of the left hand (Test 2), middle-ring fingers of the right hand (Test 3), or middle-ring fingers of the left hand (Test 4) (Fig. 2). Before the experiments, the lengths of the index, middle, and ring fingers of both hands were measured from the palmar digital crease to the fingertips on the palmar sides of the hands. To standardise the positions of the participants and manikin, the participants performed TFCC on the right side of the manikin when they used two fingers of the right hand (Tests 1 and 3) and on the left side of the manikin when they used two fingers of the left hand (Tests 2 and 4). The sequences of the tests were randomly allocated.
Fig. 2
Postures of the two-finger chest compression in the tests. Test 1: Two-finger chest compression with the index-middle fingers of the right hand. Test 2: Two-finger chest compression with the index-middle fingers of the left hand. Test 3: Two-finger chest compression with the middle-ring fingers of the right hand. Test 4: Two-finger chest compression with the middle-ring fingers of the left hand. The test 1 and 3 were conducted on the right side of the manikin and the test 2 and 4 were conducted on the left side of the manikin.

Performance data were collected using the SimPad SkillReporter (Laerdal Medical). The data included MCD (mm), total compressions (TCs, number), ratio of deep-enough compressions (DEC, %), ratio of compressions fully released (CFR, %), mean compression rate (MCR, numbers/min), hands-off time (HOT, s), total ventilations (TVs, numbers), and mean volume (MV, mL).
Outcome variables
The primary outcome variables were MCD and DEC. The other variables (TC, CFR, MCR, HOT, TV, and MV) served as secondary outcome variables.
Statistical analysis
All statistical analyses were performed using IBM SPSS v.20.0 (IBM, Armonk, New York, NY, USA). The data are presented as the means ± standard deviations. Data were analysed using the Shapiro-Wilk test to verify the normality of distribution. For normally distributed data, a two-sided paired t-test was used; otherwise, the Wilcoxon signed-rank test was used. A P value of < 0.05 was considered to indicate statistical significance.
RESULTS
Participants’ characteristics
Thirty healthcare providers (19 males, 11 females; 22 medical doctors, 8 nurses) participated in the experiment. Their mean age was 28.4 ± 3.6 years (males 29.0 ± 3.8; females 27.5 ± 3.1 years). Twenty-eight participants were right-handed and two were left-handed. The respective mean lengths of the index, middle, and ring fingers were 69.7 ± 3.5, 77.5 ± 4.3, and 71.6 ± 3.9 mm on the right hand and 70.0 ± 4.0, 77.6 ± 4.3, and 71.8 ± 4.1 mm on the left. For both hands, the length differences between the index and middle fingers were significantly greater than those between the middle and ring fingers (P < 0.01, Table 1).
Table 1
Comparisons of the length differences between the adjacent two-fingers

Comparisons of TFCC performances: right vs. left hand
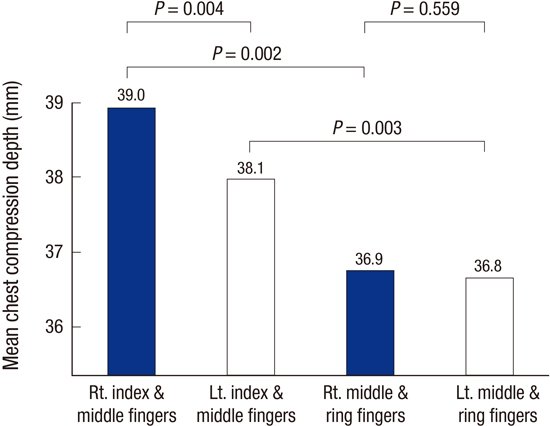
The MCDs and DECs were significantly greater when TFCC was performed with the right index-middle fingers than with the left index-middle fingers (P < 0.01, Table 2, Fig. 3). Although the MCD and DEC did not differ significantly in the TFCC performed with the middle-ring fingers, TC was significantly greater using the right than the left hand (P = 0.029, Table 2). The other variables were not significantly different.
Table 2
Comparisons of two-finger chest compression techniques: right vs. left hand


Comparisons of TFCC performances: index-middle vs. middle-ring fingers
For both hands, the MCDs and DECs were significantly greater when TFCC was performed with the index-middle fingers than with the middle-ring fingers (P < 0.01, Table 3, Fig. 3). The other variables were not significantly different.
Table 3
Comparisons of two-finger chest compression techniques: index-middle vs. middle-ring fingers

DISCUSSION
Studies of TFCC have focused on comparisons with TTHT (791011121314151617181920) and the results consistently showed the superiority of the latter technique. Although several studies have recommended TTHT, even in lone-rescuer infant CPR (1520), in one study the HOT of TTHT was significantly greater than that of TFCC (15). Another study used the over-the-head two-thumb encircling technique (OTTT) in an attempt to reduce the HOT (19), with the rescuer positioned over the head of the manikin during CPR. While the HOT did not differ significantly between OTTT and TFCC, the proportion of complete recoil was significantly lower in OTTT. These results support the use of TFCC first when a lone rescuer performs CPR for infant cardiac arrest, as stated in the recent guideline (1).
This raises the question of the proper fingers to use for TFCC. Neither the optimal finger combination nor the optimal hand for performing TFCC has been studied. In addition, recent guidelines do not include any recommendations regarding finger and hand use in TFCC (1). In the illustration of TFCC included in the 2010 American Heart Association guidelines, the rescuer used the middle and ring fingers of the right hand for TFCC (21), but this choice was neither described nor justified.
We predicted that the mechanisms of chest compression force generation would differ completely between TFCC and two-handed chest compression techniques. During TFCC, the interphalangeal joints of the two fingers should be fully extended to transfer the compression force to the fingertips. This implies that the performance of TFCC is influenced by the amount of finger strength. This study paid attention to hand grip power because stronger hand grip power might be associated with greater finger strength. Several studies have shown that the hand grip power of the right hand is greater than that of the left hand in both right- and left-handed individuals (345). We also noted that some rescuers could not perform adequately TFCC because of a much shorter index finger. This suggested that if the two adjacent fingers differ greatly in length, the performance of TFCC will be compromised.
Our study found that while the best TFCC performance was obtained using the two fingers of the right hand, TFCC performance was better with the index-middle fingers than with the middle-ring fingers, although the length difference between the index and middle fingers was greater than that between the middle and ring fingers of the participants. This might reflect the fact that the index finger is used more frequently than the ring finger. In addition, the contribution of the radial side to hand grip power is much greater than that of the ulnar side (approximately 60% and 40%, respectively) (22).
This study asked the question, “Which fingers do we perform two-finger chest compression with?” The answer is the index-middle fingers of the right hand. Although TTHT is superior to TFCC, if the latter is performed using the index-middle fingers of the right hand, it may meet the requirements of the current guidelines.
Our study had several limitations. First, the results were obtained using a mechanical model and may not be representative of real-life situations. A human clinical trial is needed to confirm our results. Second, the experiment was conducted with the manikin on the floor, because this was considered to reproduce the conditions faced by a single-rescuer performing CPR in an out-of-hospital environment. It remains to be determined whether different results would be obtained in an in-hospital environment, i.e., with the infant lying on a bed. Third, although the grip power of the right hand is stronger, even in left-handed individuals (45), the majority of the participants in our study were right handed and the results must still be confirmed in left-handed rescuers.
The best performance of TFCC in a simulation of 30:2 compression: ventilation CPR performed by one-rescuer on an infant in cardiac arrest lying on the floor was obtained with rescuers using the index-middle fingers of the right hand.
 XML Download
XML Download