

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Streptococcus pneumoniae is an important pathogen that causes morbidity and mortality in children in the first years of life, causing clinical syndromes varying from mucosal disease (sinusitis and otitis media) to invasive pneumococcal diseases (IPD; e.g., sepsis and meningitis) (1). To prevent pneumococcal infections in young children, the 7-valent pneumococcal conjugate vaccine (PCV7, PrevenarTM, Pfizer Inc, Philadelphia, PA, USA), which includes serotypes 4, 6B, 9V, 14, 18C, 19F and 23F, was licensed in the USA in 2000 and has been recommended for inclusion in national immunization programs for young children (2). Following the introduction of PCV7 overall IPD rates among children aged < 5 years in USA were reduced by 77% compared with the prevaccine era (3).
Pneumococcal conjugate vaccines provide serotype-specific protection against vaccine serotypes (VTs) and some vaccine-related serotypes (VRTs) of S. pneumoniae (45). There have been some reports of enhanced cross-reactivity according to the number of vaccinations (67). In children under 24 months of age, 3 primary doses of immunizations with PCV7 elicited immune responses for serotypes 6B and 6D, and a booster dose enhanced cross-reactive immune responses against serotypes 6A, 6C, and 6D (6). In addition, while the cross-reactive immune response against serotype 19A appeared in only a small proportion of subjects after a primary series of 3 doses, it was amplified after the booster vaccination (89).
Although antigen-specific serum IgG antibodies have been used as a surrogate marker demonstrating vaccine-induced protection against many diseases, IgM is the first antibody produced in a humoral immune response because it can be expressed without isotype switching. IgM mostly exists as a pentamer whose ten antigen binding sites can bind simultaneously to multivalent antigens such as bacterial capsular polysaccharides (PSs). This structure results in high avidity despite its relatively low affinity. Moreover, IgM can be particularly effective at complement activation (10). Indeed, studies with human monoclonal antibodies have shown that IgM antibodies are more efficient for opsonophagocytic killing of bacteria than IgG antibodies (1112).
Previous studies have demonstrated the role of serotype-specific IgM antibodies on the immunogenicity of the pneumococcal vaccine in adults and children (1314). IgM antibodies could be involved in cross-protection against VRTs, but the role of cross-protective IgM antibodies has not been investigated previously (68). Therefore, we aimed to investigate the impact of IgM on cross-protection against serotypes 6A, 6C, and 19A in children after booster immunization of PCV7.
MATERIALS AND METHODS
Subjects
Serum samples were obtained one to three months after the last vaccination from 18 healthy children aged 12 to 23 months immunized with PCV7 at 2, 4, and 6 months and after 12 months of age. All serum samples were stored frozen at -70°C until analysis. Written informed consent was obtained from parents or legal guardians following a detailed explanation of the study.
Enzyme-linked immunosorbent assay (ELISA)
The IgG antibody concentrations against serotypes 6B and 19F were measured by the third-generation pneumococcal antibody ELISA posted on a website (http://www.vaccine.uab.edu), but the ELISA was modified for measuring IgM antibody concentrations as previously described (13). The ELISA was performed at the Center for Vaccine Evaluation and Study, Ewha Medical Research Institute at Ewha Womans University.
Opsonophagocytic killing assay (OPA)
The opsonic activities of the serum samples for two vaccine serotypes (6B and 19F) and three vaccine-related serotypes (VRTs; 6A, 6C, and 19A) were evaluated by OPA, as previously described (151617). The opsonic index (OI) was defined as the serum dilution that killed 50% of bacteria and was determined by linear interpolation. In this study, all serum samples were diluted 40-fold before the assay due to limited amounts of serum. Because all serum samples were diluted 4-fold during the assay, the limit of detection was 160. A detailed protocol is posted online (http://www.vaccine.uab.edu).
Depletion of IgM from immune serum by affinity chromatography
To remove IgM antibody from immune serum, the serum samples were mixed with agarose beads conjugated with anti-human IgM antibody (Sigma-Aldrich, St. Louis, MO, USA) and incubated for 2 hours at RT. Unconjugated agarose beads were used as a control. The mixtures were applied to Bio-Rad chromatography spin columns (Bio-Rad Laboratories, Inc., Hercules, CA, USA). The columns were centrifuged at 2,000 r.p.m. for 1 minute at 4°C, and the eluted fraction was collected. The efficiency of depletion was monitored using the pneumococcal antibody ELISA. The optical density was measured at 405 nm to determine the concentration of anti-pneumococcal PS (anti-PnPS) IgM antibody in the 1:1,000 diluted absorbed serum (13).
Statistical analysis
The geometric means of OIs (GMIs) against serotypes 6B, 19F, 6A, 6C, and 19A in IgM-depleted immune serum and control serum samples were analyzed by IBM SPSS Statistics 21 (IBM Corporation, Armonk, NY, USA). Comparisons of anti-PnPS IgG and IgM concentrations and OIs between IgM-depleted serum and control serum were performed with a Wilcoxon signed-rank test, and P values < 0.05 were considered statistically significant. Values below the limit of detection were substituted with the half of the limit of detection. The interquartile range (IQR) of OIs between IgM-depleted serum and control serum was estimated, except in samples showing an OI lower than the detection limit of the OPA.
RESULTS
Effects of IgM depletion on opsophagocytic activities against serotypes 6B and 19F
Anti-PnPS IgG and IgM antibody concentrations and OIs for serotypes 6B and 19F are displayed in Table 1. In Fig. 1, the OI for each serum is plotted against its respective anti-PnPS IgG and IgM antibody concentration.
Table 1
IgG and IgM antibody concentrations and opsonic indices against serotypes 6B and 19F in children after booster immunization with PCV7
Fig. 1
Distribution of the opsonic indices and serotype-specific IgG or IgM concentrations. (A) serotype 6B, (B) serotype 19F.

To investigate the role of anti-PnPS IgM antibodies in the opsonic capacity of the immune serum, IgM was removed by affinity chromatography from immune serum and the depleted immune serum were tested by OPA for serotypes 6B and 19F. IgG and IgM antibody concentrations for serotypes 6B and 19F in IgM-depleted immune serum and control serum were determined by ELISA to determine the efficiency of depletion. Affinity chromatography resulted in minimal loss of IgG antibodies for serotypes 6B and 19F, but removed a significant proportion of IgM antibodies for the same serotypes (Fig. 2). When the opsonophagocytic activities were determined by OPA in IgM-depleted immune serum and control serum, geometric mean opsonic indices (GMIs) decreased from 3,009 (95% CI: 1,001-9,042) in control serum to 1,396 (95% CI: 520-3,749) in IgM-depleted serum for serotype 6B. Each immune serum showed a 38% (median, interquartile range [IQR] 26%-67%) reduction of OIs against serotype 6B by IgM depletion. For serotype 19F, GMIs decreased from 1,117 (95% CI: 364-3,436) in control serum to 750 (95% CI: 285-1,973) in IgM-depleted serum. Each immune serum showed a 36% (median, IQR 0%-51%) reduction of OIs against serotype 19F by IgM depletion (Fig. 3).
Fig. 2
Comparison of the changes in IgG and IgM concentrations in response to vaccine serotypes in PCV7 immune serum after IgM depletion. (A) anti-PnPS 6B IgG and IgM concentrations in control serum and IgM-depleted serum, (B) anti-PnPS 19F IgG and IgM concentrations in control serum and IgM-depleted serum.

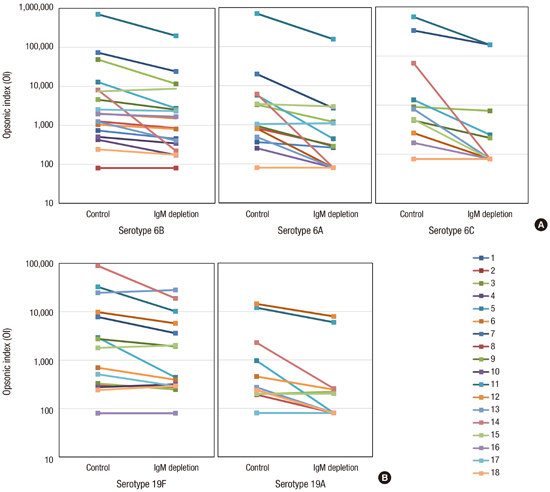
Fig. 3
Reduction of opsonic indices to vaccine serotypes and vaccine-related serotypes in PCV7 immune serum after IgM depletion. (A) Opsonic indices against serotypes 6B, 6A and 6C in control serum and IgM-depleted serum. (B) Opsonic indices against serotypes 19F and 19A in control serum and IgM-depleted serum.
Effects of anti-PnPS 6B and 19F IgM antibodies on cross-protective activities for serotypes 6A, 6C and 19A
To investigate the contribution of anti-PnPS IgM antibodies to cross-protective activities for VRTs in the immune serum, we measured the OIs of IgM depleted immune serum and control serum against serotypes 6A, 6C, and 19A.
The GMIs against serotype 6A were 961 (95% CI: 294-3,143) in control serum and 329 (95% CI: 121-891) in IgM-depleted serum, representing a 3-fold decrease in GMIs and a 70% (median, IQR 64%-87%) decrease in OIs in each immune serum. The GMIs against serotype 6C were 432 (95% CI: 149-1,247) in control serum and 185 (95% CI: 77-441) in IgM-depleted serum, representing a 2-fold decrease in GMIs and a 72% (median, IQR 54%-83%) decrease in OIs in each immune serum. The GMIs against serotype 19A were 301 (95% CI: 132-688) in control serum and 166 (95% CI: 82-337) in IgM-depleted serum, representing a 2-fold decrease in GMIs and a 58% (median, IQR 46%-68%) decrease in OIs in each immune serum (Fig. 3).
DISCUSSION
This study demonstrates that the PCV7 booster elicits protective antibodies in the form of IgG and IgM, and that IgM antibodies contribute to cross-functional opsonophagocytic activities against VRTs 6A, 6C, and 19A. Previous studies reported that the booster immunization of PCV7 for children aged 12-23 months induces cross-protection against serotypes 6A, 6C, and 19A (68). However, the serological properties of cross-protective antibodies against these VRTs obtained from PCV7 immunization were not investigated. This study is the first attempt to study the role of IgM antibody in cross-protection against VRT pneumococci. IgM antibodies are predominantly elicited in a T cell-independent immune response by PS antigens that are not processed and presented by MHC molecules. Because PS antigens do not activate follicular B cells but directly activate mature B cells without T cell help, they do not undergo affinity maturation and Ig class switching. Consequently, they elicit predominantly low-affinity IgM antibodies and fail to develop immunological memory (10). Nevertheless, some studies showed roles for IgM in opsonic activity and immune memory by enhancing avidity and ability to trigger the complement system, and by generating T-cell dependent IgM memory B cells (1819).
Although conjugate vaccines mainly produce IgG through a T-cell dependent immune response, all subjects in this study obtained high concentrations of IgG and IgM antibodies and good functional immune responses to serotypes 6B and 19F after the booster immunization of PCV7. In addition, opsonic activities against serotypes 6B and 19F in each subject were related to the existence of IgM. This is consistent with previous reports about the role of IgM in the immunogenicity of the pneumococcal vaccine. A recent study in adults showed that PPV23 is less effective for older adults than for young adults, mainly due to low serotype-specific IgM antibody levels in older adults (13). In another toddler study, the correlation between IgM antibody concentrations and opsonic activities was stronger than that of IgG antibodies after a single dose of PCV9 vaccination. In that study, OPAs against serotype 14 remained in pooled serum samples after IgG depletion and was assumed to relate with the concentration of anti-PnPS 14-specific IgM antibody (14). This study attempted to investigate the relationship between IgM antibody and OPA against VRTs using IgM depletion. IgM depletion led to a marked decrease in the opsonic capacities against serotypes 6A, 6C and 19A without considerable changes in IgG concentrations of immune serum. These results show that IgM antibodies influence functional opsonophagocytic activities against VRTs, such as serotypes 6A, 6C, and 19A.
Because some IgM antibodies are not only protective against bacterial infections but also bind many unrelated antigens, such as single-stranded DNA, thyroglobulin, and β-galactosidase, such IgM antibodies are called polyreactive or natural antibodies (20). However, high opsonic IgM antibodies in immune serum after PPV23 vaccination in the elderly are not reduced by the existence of single-stranded DNA, thyroglobulin, and β-galactosidase. In addition, opsonic activities against VRTs were totally inhibited in IgM-depleted immune serum and control serum mixed with free 6B or 19F polysaccharide antigen (data not shown). Therefore, IgM antibodies specific for VTs seem to be also reactive with VRTs, rather than polyreactive.
There have been some reports on the possible role of IgM in protection against other pathogens. Functional antibody activities induced by Haemophilus influenzae type b conjugate vaccine were related to both anti-PRP IgM and IgG concentrations (21). In regard to the Salmonella typhi vaccine, repeated antigen exposure with S. typhi porins could promote the generation of protective IgM antibodies (22). IgM antibodies induced by meningococcal polysaccharide vaccine could contribute to functional antibody activities against group C meningococcus, despite its small quantity (23).
It has been noted that the correlations between opsonophagocytic activities and IgG concentrations were lower for VRTs than for VTs (924). This study demonstrated substantial roles of IgM in cross-protection against VRTs as well as in opsonic capacity against VTs. Considering these data, evaluation of functional immune response using the OPA would be more desirable than an ELISA measuring only IgG antibodies, especially for evaluation of immunogenicity to VRTs (21).
Compared to studies in infants from the USA, Europe, or Taiwan, Korean infants had higher post-vaccination antibody titers to all serotypes in PCV7 (25). In addition, Korean children had higher post-vaccination opsonic indices than children in other countries against all serotypes in PCV7 and two VRTs (serotype 6A and 6C) (unpublished data). Higher immunogenicity in Korean children could develop due to a difference in IgM antibody responses among ethnic groups.
This study suggests that IgM antibodies contribute to the functional antibody response against VRTs as well as VTs in young children. However, this study was a small study performed on a limited sample size based on the immune responses to PCV7, and there were no post-primary vaccination immune serum available. In addition, new conjugate vaccines containing more serotypes and different carrier proteins were recently developed, and some conjugate vaccines were approved for adults (262728). Further studies are needed for more subjects including children and adults, as well as for different vaccine formulations. Moreover, studies in different populations or ethnic groups will provide better information for understanding immune response by pneumococcal vaccine.
In conclusion, the booster immunization PCV7 induced protective antibodies in the form of both IgG and IgM isotypes, and elicited cross-protection against serotypes 6A, 6C, and 19A among Korean children. IgM antibodies induced by PCV7 contribute to opsonization of serotypes 6A, 6C, and 19A.
 XML Download
XML Download