

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The increasingly rapid transition to an aging and aged society, as marked by increased numbers of elderly due to prolonged average life spans, is now a global phenomenon, and Korea certainly is no exception in this regard. As a principal component of the necessary establishment of comprehensive elderly persons' health and welfare policies in Korea, from July 2008, a long-term care insurance system has covered those who are rated as requiring long-term care (1). These individuals are persons aged at least 65 yr or those aged less than 65 yr but who for some reason cannot perform activities of daily living alone for more than six months due to conditions such as dementia and cerebrovascular diseases. These people are at very high risk of falls due to pain from chronic diseases, reduced lower-extremity muscle strength, and joint system diseases, along with the progression of physiological aging (23). Since the number of elderly persons living in nursing homes has recently increased, studies are needed on falls of patients with a relatively high fall risk, particularly those involving hip fractures, from which high mortality and low rates of recovery of the capacity for activity can be expected (4). However, neither has related information been collected nor have related studies been conducted in Korea.
Therefore, the authors conducted the present study to examine the risk factors for hip fracture, the degree of recovery of the capacity for activity, and the mortality rates among those with hip fractures occurring in nursing homes.
MATERIALS AND METHODS
Subjects
The present study was conducted with 46 patients who had suffered a hip fracture (46 accidents, 1.25% of residents, 15.4% of fall-accident victims) among 299 patients who had experienced a fall accident (371 accidents, 7.6% of residents) out of a total of 3,949 residents who had been admitted to one of five nursing homes between August 24, 2008 and January 31, 2014. The mean age of the patients was 82.7 yr (66-94 yr), and there were 28 males and 18 females. To examine differences in hip-joint-fracture risk factors, the rate of recovery of the capacity for activity after fracture and mortality rates, a nursing home residents (NHR) group was compared with community-dwelling individuals (CDI), a control group of the same number of subjects.
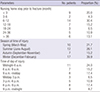
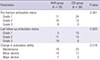
Fractures were divided into femoral neck fractures and intertrochanteric fractures according to location; and fracture types were subdivided using the Garden classification (5) and the AO classification (the Association for Osteosynthesis/Orthopaedic Trauma Association [AO/OTA] classification). The NHR group comprised 21 left hips with a fracture and 25 right hips with a fracture; among them all, 14 hips (30.4%) involved a femoral neck fracture and 32 (69.6%), an intertrochanteric fracture. In the subdivision by fracture type, Garden classification (5) type 3 was the most frequently occurring (10 hips) among the femoral neck fractures, while AO classification type 2 was the most frequent (22 hips) among the intertrochanteric fractures (Table 1). Radiologic measurement and evaluation for fracture classification were conducted by two orthopedic surgeons based on antero-posterior and lateral radiographs of the hip joint. Kappa coefficient tests were applied to measure the intra-observer (K1) and inter-observer (K2) reliability of the two observers; both sets of results were shown to be at reliable levels (K1=0.88, K2=0.81). Seven patients (15.2%) in the NHR group did not undergo surgery. These hips included one wherein surgery was not possible due to health condition, and six in which surgery was not performed owing to the family's refusal. In the CDI group, one patient, for health reasons, did not undergo surgery (P=0.026). The surgery waiting time in the NHR group's 39 hips in which surgical treatment was performed was not longer than one week in most hips (36 hips). Among the surgical methods, proximal femoral nailing was the most frequent, in 21 hips, and anesthesia was administered by general anesthesia in 23 hips and by spinal anesthesia in 16. The mean hospitalization period was 34.3 days (minimum 7 days, maximum 104 days); patients for whom the hospitalization period was 30 days or longer were the most common (16 hips). The surgery waiting time, surgical method, and hospitalization period within the NHR group were not significantly different than in the CDI group (Table 1).
The degree of capacity for activity before hip fracture and at final post-fracture follow-up was classified into three levels. Level 1 was defined as cases wherein the patient could perform activities alone or use walking-assistance tools (cane, walker) without being helped by others (independent ambulator); level 2 were cases in which the patient could perform activities only when helped by others (dependent ambulator); level 3 cases were those in which the patient could not conduct any activities other than moving in a wheelchair or resting in bed (non-functional ambulator). The capacity for activity and death were evaluated by retrospectively collecting information from hospital records, nursing home records, and phone calls to patients or their lineal family members. When information could not be easily obtained from patients or their lineal family members or patients could not be contacted in the process of the survey, contact information could be obtained with the help of government offices in order to determine accurately whether the patients had died or not and, in cases of death, when the death had occurred.
Analysis of external factors related to hip fracture patients in nursing homes
The period of time from the date of admission to the nursing home and the date of injury, along with the season and time of injury of each patient, were examined. The seasons of injury were divided into March through May (spring), June through August (summer), September through November (autumn), and December through February (winter); the time of injury was divided into three-hour intervals except for the period from 24:00 to 06:00, which was established as a single time period (sleeping time).
Analysis of internal factors related to NHR and CDI
Age, weight, height, body mass index (BMI), the capacity for activity before injury, and any comorbidity possibly influencing patients' falls were examined. Comorbidity was evaluated by determining whether the fracture was accompanied by any lung disease, cerebrovascular disease, cardiovascular disorder, hypertension, diabetes, Parkinson's disease, or dementia.
Evaluation of recovery of capacity for activity of NHR and CDI
Considering the typical characteristics of patients admitted to nursing homes, it was thought important to examine the state of mobility immediately before death in cases where the patient died within a short period after hip fracture. Therefore, the capacity for activity at final follow-up was examined in all cases, and patients who survived for at least one year underwent additional analysis. Changes in the capacity for activity were divided into maintenance, minor decline (one-level decline), and major decline (from independent ambulation to non-functional ambulation) so as to examine changes from before hip fracture to the time of final follow-up. The associations between age, fracture type, and comorbidity possibly affecting recovery of either capacity for activity or capacity for activity prior to hip fracture were examined.
Analysis of rates of death of NHR and CDI within one year
Those who died within one year of hip fracture were analyzed. Patients' age, BMI, comorbidity, number of accompanying diseases, whether the patient had dementia or not, fracture type, whether the patient underwent surgery or not, and changes in the capacity for activity that were considered to have possibly influenced death were examined. For comparison of mortality rates between the NHR group and the CDI group, survival analyses were conducted.
Analysis of disputes raised after occurrence of hip fracture in nursing homes
The kinds and contents of disputes occurring between patients or their family and nursing homes after the occurrence of hip fracture were examined. The kinds of disputes and resolution processes were analyzed based on public-record documents and insurance-related documents kept in the nursing homes.
Statistical analysis
A control group (CDI) was organized by selecting a group with the smallest difference in age, specifically by repeating propensity-score matching processes (matched-pair analysis performed 100 times) with patients selected based on age (at least 65 yr old) and gender from those who visited the emergency room of this hospital due to hip fracture while living at home (excluding pathological fractures and bilateral fractures). Kaplan-Meier survival analyses were conducted using death within one year as the end point as well as Student's t tests and chi-square tests for comparisons between the two groups and comparisons between the dead and survivors within each group. For the NHR group, factors that were considered to have affected the capacity for activity and death within one year were analyzed by logistic regression using SPSS 18.0 (Chicago, IL, USA). Differences wherein the P value was smaller than 0.05 were considered to be statistically significant.
RESULTS
Analysis of external factors related to nursing home hip fracture patients
The mean period of time from the date of admission to the nursing home to the date of fracture was 484.2 days (minimum 2 days, maximum 1,925 days). Fractures occurred the most frequently (14 hips; 30.4%) during the period between six months and 12 months after admission. The classification of fracture by season revealed that fractures occurred the most frequently (17 hips; 36.9%) between December and February. With regard to the time of injury, fractures occurred the most frequently (11 hips; 24%) between 24:00 and 06:00; the incidence rate was highest (22 hips; 47.9%) between 21:00 and 09:00, the time considered to correspond most closely to the sleeping period (Table 2).
Analysis of internal factors related to nursing home hip fracture patients
Among the patients, males and females had fractures that involved 28 and 18 hips, respectively. The mean age was 82.7 yr (minimum 66 yr, maximum 94 yr), and those in their 80s were the largest in number at 31 cases. The mean BMI was 19.9 kg/m2 (minimum 15.7 kg/m2, maximum 32 kg/m2). The BMIs were divided into three levels for the analysis (level 1, lower than 18.5; level 2, 18.5-22.9; level 3, 23 or higher): 18 hips were at level 1, 19 at level 2, and 3 at level 3. According to the evaluation of the capacity for activity before hip fracture, dependent ambulators were the largest in number, at 22 cases. Of the total 46 cases, 27 were dementia patients; among the other accompanying diseases, hypertension was shown to be the most common (29 cases) (Table 1).
Comparative analysis of hip-joint-fracture risk factors and fracture types in NHR and CDI
In both groups, intertrochanteric fractures occurred more frequently than other types of fractures; and there was no significant difference in fracture types between the two groups. The NHR group showed significantly lower BMIs (P=0.002) and capacity for activity before hip fracture (P=0.002) as well as significantly more cases of cerebrovascular disease, Parkinson's disease, and dementia. The cases wherein the number of accompanying internal-medicine diseases was 3 or larger (P=0.828) and those in a high-risk group with an ASA score for physical status before surgery of 3 or more (P=0.460) were larger in the NHR group, though the differences were not statistically significant (Table 1).
Evaluation of capacity for activity of all NHR and CDI
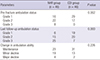
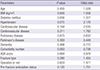
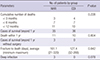
Among the 46 subject patients in the NHR group, the level of capacity for activity was maintained in 23 patients, dropped by one level in 19, and dropped by two levels in four. In the CDI group, the levels were maintained in 31, dropped by one level in 13, and dropped by two levels in two. The differences between the two groups were not statistically significant (P=0.226). However, the number of non-functional ambulators increased by 7 in the CDI group and by 17 in the NHR group, reflecting significant declines in the capacity for activity (P=0.000) (Table 3). Logistic regression analyses were conducted at final follow-up in order to determine and analyze the factors affecting such declines. Based on the results of the analyses, it was concluded that hypertension (P=0.075, odds ratio, 2.176) or multiple accompanying diseases (P=0.083, odds ratio, 1.687) could affect the declines, though their effects were not statistically significant (Table 4).
Evaluation of capacity for activity of those among NHR and CDI who survived for at least one year
Among the patients in the NHR group, 35 survived for at least one year after hip fracture, while the capacity for activity was maintained at final follow-up in 19, declined by one level in 15, and declined by two levels in one case. In the CDI group, 36 survived for at least one year after hip fracture in the CDI group, while the capacity for activity was maintained at final follow-up in 23, declined by one level in 11, and declined by two levels in two (P=0.518). The differences in these changes within the NHR group were not statistically significant. However, in the evaluation of the capacity for activity at the final follow-up, the NHR group showed significant declines (P=0.002) as well as an increase of 11 in the number of non-functional ambulators, while the CDI group showed an increase of only 6. This significant difference was attributed to the larger number of dependent ambulators prior to hip fracture in the NHR group (P=0.001) (Table 5).
The analysis of factors that could affect declines in the capacity for activity in the NHR group indicated that the capacity for activity had significant effects (P=0.041, odds ratio , 2.996) and that accompanying cerebrovascular diseases were highly likely to have effects, though this result was not significant (P=0.12, odds ratio, 3.025) (Table 6).
Evaluation of mortality rates of NHR and CDI within one year of hip fracture
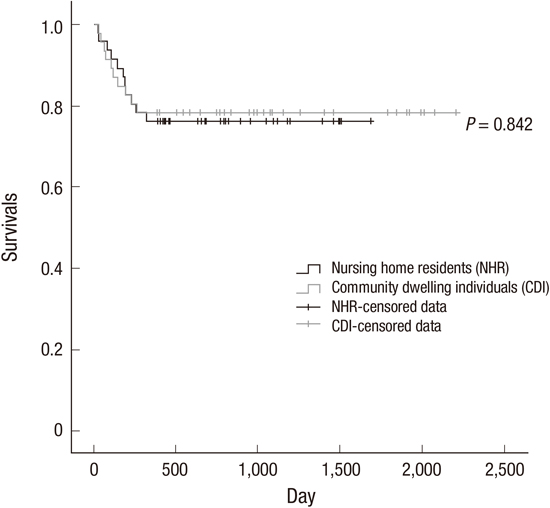
In the NHR group, 11 patients died within one year (23.9%), and among them, death occurred a mean of 161.1 days (minimum 21 days, maximum 320 days) after hip fracture. The cumulative number of deceased patients by period was 3 within three months, 7 within six months, and 11 within 12 months. In the CDI group, 10 (21.7%) died within one year after hip fracture; and among them, death occurred a mean of 127.4 days (minimum 32 days, maximum 266 days) after hip fracture. The cumulative number of deceased patients by period was 4 within three months, 7 within six months, and 10 within 12 months. Kaplan-Meier survival analyses of the two groups showed no significant differences between them (P=0.842) (Fig. 1) (Table 7).
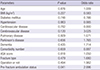
According to the comparison between those who died within one year and those who survived (35 hips, 76.1%) in the NHR group, patients' age, comorbidity, and fracture type had no relationship with survival. However, although not statistically significant, whether the patient underwent surgery or not (P=0.097, odds ratio, 4.571) and a decline in the capacity for activity (P=0.07, odds ratio, 2.705) were considered highly likely to have a significant relationship. Additionally, logistic regression analyses of the risk of death within one year indicated that on the basis on an odds value of 1, the risk of death of patients with hypertension was approximately 2.6 times higher, and that of patients with cardiovascular diseases was approximately 2.8 times higher. There were three cases where the patient did not undergo surgery but survived for at least one year. Of these, two were non-functional ambulators before fracture and Garden classification type 1 and type 4 femoral neck fracture patients, respectively, and the remaining single case was an independent ambulator before fracture who became a non-functional ambulator after fracture (and had an AO classification type 2 intertrochanteric fracture) (Table 8). The three cases of postoperative infection that could have affected death within one year all occurred in the NHR group (P=0.078) (Table 7). Of these, two patients survived for at least one year after removal of artificial joints in the final surgery, though the remaining one patient who had undergone cement spacer insertion under a planned two-stage replacement died within one year.
Analysis of disputes that were raised after occurrence of hip fractures at nursing homes
Among the patients who had hip fractures that occurred in nursing homes, insurance companies that had contracts with nursing homes compensated patients and their family members in 32 cases (69.6%). Patients' family members raised civil complaints or filed lawsuits against nursing homes in 41 cases. The contents of civil complaints (41 cases) and lawsuits (2 cases) overlapped in the evaluation, and among them, claims for nursing expenses during hip fracture treatment (37 cases) and complaints about caregivers in nursing homes (27 cases) were the most frequent; there also were complaints about initial responses to non-functional ambulators because fractures had been overlooked for several days (3 cases). In light of the fact that the civil complaints included many indicating that after hip fracture, the patient could not be adequately treated at hospitals or at nursing homes (22 cases), the period after fracture and before being readmitted to a nursing home to start living there again (the period before nursing home readmission) was examined among patients who survived for at least one year. The period before readmission was classified into four levels: 7 days or less, 8-14 days, 15-28 days, and 28 days or more. Cases of 15-28 days were the most frequent (11 patients). Patients who survived for at least one year were divided into those with at least one-level declines ("any decline") in the capacity for activity and those with no decline, in order to determine whether the readmission period was related to a change (a decline in all cases) of any kind. Of the 35 patients who survived for at least one year, 16 showed at least one-level declines along with significantly shorter periods before readmission (P=0.015). Additionally, logistic regression analyses indicated that the period before readmission was related to declines in the capacity for activity (P=0.009, odds ratio, 7.277).
DISCUSSION
Because most patients living in nursing homes are elderly, have comorbid conditions, and have inadequate ambulatory abilities from reduced muscle strength, they are at high risk of falls. According to international research, hip fractures are known to be the most common type of falling accident in nursing homes (6). However, necessary information and studies related to this subject are lacking in Korea, which has motivated this study.
Out of the total 3,949 residents who had been admitted to 5 different nursing homes, 299 residents (371 incidents) had falling accidents, and among them, 46 residents (46 incidents) suffered hip fracture. These fractures accounted for 15.4% of the total fall accidents and 1.25% of the total residents. The incidence of falling accidents in this study was lower than that of the previous study (7) conducted on elderly persons in nursing homes in Korea, which was reported to be 30.3%. The difference between the incidences was presumably because the previous study had surveyed the experience of falls without considering the fall severity, whereas the present study did not include light falls from the records of nursing homes.
In terms of evaluation of functional recovery after the hip fracture, no standardized method has yet been established for evaluating the level of ambulatory ability as well as functional recovery based on differences in the fracture location, the treatment method, and the time of evaluation; however, one study from outside Korea reported functional recovery in 41%-97% of cases (8), and a Korean study reported a diverse range of functional recovery of 33%-68% (910). Considering the specificity of individual residents of nursing homes, that is, the fact that the residents walk mainly with the assistance of canes, walkers, or another person rather than independently, the authors classified the capacity of activity before and after hip fracture into three levels: independent ambulation, dependent ambulation, and non-functional ambulation. According to the retrospective evaluation of the pre-injury capacity of activity of the total 46 residents, only 16 were independent ambulators, meaning that many patients had reduced ambulatory capacity, and 4 were non-functional ambulators who suffered hip fractures as they had fallen out of bed while another person had been changing the subject's position or clothes. These findings emphasize that extra attention devoted to the basic nursing care of non-functional ambulators living in nursing homes is needed. When the patients who survived for at least one year after hip fracture were analyzed, 6 out of the 11 patients who had been independent ambulators before the injury had become dependent or non-functional ambulators, which implies that many patients (6 subjects, 54.5%) who had been independent ambulators before hip fracture were unable to recover their prefracture ambulation ability.
Consequently, the authors conclude that when patients who had been able to function independently or move using walking aids without any assistance from others have suffered a hip fracture, greater attention towards both surgery and rehabilitation treatment are necessary to help these patients recover prefracture ambulation capabilities. Furthermore, examinations indicated that those who had limited ambulatory ability before hip fracture or those who had comorbid cerebrovascular disease showed a great decline in their ambulatory ability after hip fracture; thus, evaluation of patients' basic daily activities including the subjects' ambulatory abilities as well as their medical conditions before the patients are admitted to the nursing home are necessary. The authors did not find that the most prominent diseases of cognitive impairment such as Alzheimer's disease and Parkinson's disease had a statistically significant relationship with the decline of the patient's functioning after hip fracture; however, since cognitive impairments greatly interfere with the rehabilitation process after surgery and therefore may negatively affect the recovery (11), changes in cognitive ability before and during admission should also be carefully evaluated.
The mortality rate within one year after hip fracture has been previously reported to be 10%-36% (12); however, Kim et al. (13) have recently reported that because earlier studies in Korea on the mortality rate were based only on the patients who had been under follow-up for a certain period of time, the actual mortality rate is expected to be much higher than reported, and that the actual mortality rate of patients aged 65 yr or more within one year of hip fracture was 28.8%. In the study investigating the mortality rate after hip fractures specifically occurring in nursing homes, Berry et al. (12) reported a high mortality rate of 150 patients (76.9%) during a mean follow-up period of 1.4 yr among 195 patients (153 females and 42 males).
In particular, they reported that the mortality rate within one year after hip fracture was higher among males (53.3%) than females (35.6%) and that this could be due to the greater incidence of infection (15) and delirium (14) among male patients. In this study, 11 (23.9%) of the 46 patients died within one year after hip fracture, showing a lower mortality rate than that reported by Berry et al. (14) and similar results to previously known mortality rates after hip fracture (1213). These differences may have arisen because the study by Berry et al. (14) had been conducted in the United States, where medical insurance coverage is relatively more difficult to obtain than in Korea, where the present study was conducted; however, because various factors such as the differences in the subject groups are related to the mortality rates, further investigations must be undertaken in the future.
To prevent falling accidents in nursing homes and hip fractures from falls, important interventions include analyzing and changing the drugs or environmental factors that may cause falling accidents, as well as following an exercise therapy program to strengthen the muscles of patients with a high risk of falling, and using a hip protector (16). Following the enactment of the Act on Long-Term Care Insurance for Senior Citizens (1) in July of 2008 in Korea, 121,774 patients have been living in approximately 2,500 nursing homes as of 2013 (17). To ensure management excellence in nursing homes, the Korean government conducts evaluations of nursing homes every 3 yr and runs an incentive program providing payment of differential benefits based on the evaluation results. However, what the authors discovered in the process of research is that such evaluation is very formal and cannot sufficiently evaluate the quality of nursing homes. The current evaluation items (18) include determining patients with a high risk of falling in order to prevent falling accidents and checking facilities to prevent falls, recordkeeping of falling accidents, as well as checking insurance contracts for coverage of falling accidents.
In reality, the number of falling accidents at a particular nursing home, the presence of fractures after injury, and the diagnosis and treatment process for the fractures are not included among the evaluation items; therefore, it is problematic that the evaluation cannot provide necessary information to enable patients and guardians to assess the quality of patient care and management of the nursing homes. Consequently, the authors concluded that the allocation of duties to personnel in the nursing homes, evaluation of their professional specialty, physical space for rehabilitation, and the presence of a patient advocacy program or environmental changes to prevent falls should also be included as important items in the evaluation of the standard practices of nursing homes conducted by the Korean government. Furthermore, in the third case among those included in this study, the patient suffered a hip fracture but did not receive immediate diagnosis and medical treatment. Because a previous study (19) reported that short-term mortality within 30 days increases by 2.5 times if appropriate treatment is delayed by 4 days or more, evaluation regarding how nursing homes take measures immediately after a falling accident-in other words, whether there is a reporting system for the first detector of the fall, first aid steps to prevent additional damage, as well as a system and its manual for transfer to a medical institution for appropriate diagnosis and treatment-should also be considered important.
However, this study has limitations in that it has a small number of subjects. The reason is that although each nursing facility has records on falling accidents and hip fractures, it was difficult to recruit subjects because these data were not open to public, and the nursing homes did not provide access to the data given their concern about any possible liability they may face. Despite these limitations, the significance of this study lies in the following factors: first, it has set a reference point to compare each nursing facility in Korea by being the first to report an incidence of 1.25% of hip fractures in nursing homes in Korea. Second, it emphasizes important points that require further attention in the management of patients by analyzing and reporting the risk factors of hip fractures such as time of admission and time of fall. Third, this study has been the first to report that following the occurrence of hip fracture in nursing homes, the mortality rate within one year is not significantly different from that outside nursing homes.
When a hip fracture occurs in a nursing home, hip-related functionality deteriorates remarkably, leading to poorer quality of life for the remainder of the patient's life, which is not different from patients who suffer a hip fracture outside a nursing home; thus, when hip fracture occurs in nursing homes, the facility management should be more active in taking further steps toward correct diagnosis and treatment. Through this study, the authors have presented evidence to support that when the government conducts an assessment of nursing homes, they should include the incidence of falling accidents in the nursing homes and the resulting hip fractures that greatly affect ambulatory ability and mortality; not only is disclosing such information needed to guide nursing homes to perform extra care on patients, but systematic changes are also needed to allow users to have access to this information so that they can select good-quality nursing homes.



 XML Download
XML Download