

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Prostate cancer (PC) is currently the fourth most common male cancer in Korea (1). The annual incidence rate of PC in Korean men has been the most rapidly increasing except thyroid cancer in recent decades (2). Multiple reasons including population aging, westernization of diet and increase of prostate-specific antigen (PSA) screening are implicated in such increase of PC in Korea. PSA screening in Korea has increased with increase of routine health check-up compared to the past (34), although clinical benefit of routine PSA screening remains controversial (567).
The causes of death in PC patients may be complicated by non-PC causes as well as PC. Patients undergoing curative therapy such as surgery and radiation therapy (RT) are likely to die of non-PC causes, whereas significant proportions of patients treated with primary androgen deprivation therapy (ADT) undergo disease progression and ultimately die of PC, while some of patients die of associated comorbidities. Patients undergoing active PC treatments are also at risk for developing treatment-related comorbidities and subsequent malignancies. For example, patients undergoing ADT are at increased risk for cardiovascular disease (CVD) and osteoporosis (8910), and PC survivors remain at risk of subsequent malignancies and the types of secondary primary cancer depend on the treatment method (1112). Conversely, some cancer survivors may develop secondary PC. Because PC is a highly prevalent disease and has public health impact, many studies based on western populations have examined the importance of causes of death in PC patients (13141516), while several studies have shown changing trends in competing causes of death in PC patients (1718). In contrast, despite high prevalence and rapid increase in incidence of PC, there are few studies regarding this issue in Asian population. In this study, we investigated the causes of death in Korean men with PC and their time trends over 8 years from a nationwide population based cohort.
MATERIALS AND METHODS
Data sources
In South Korea, virtually all Koreans (97%) are covered by National Health Insurance (KNHI) (19). We obtained data from 2002 to 2010 from KNHI Sharing Service provided by KNHI Center. This data contains claims data in 2% of the entire Korean population that are randomly selected after stratifying the entire population according to socioeconomic parameters (age, sex, residential area, income, etc.). The database includes detailed information regarding disease diagnosed, laboratory tests, treatments (both medical and surgical) and death outcomes as well as aforementioned socioeconomic parameters.
Data with the code C61, which indicates PC according to the National Center for Health Statistics International Classification of Diseases, 10th edition (ICD-10), were screened. Among 3,333 men aged 20 or older with the code C61 during study period, newly diagnosed PC patients only from 2003 until 2010 were included to minimize confounding effects due to pre-diagnosed PC. In addition, to minimize confounding effects due to diagnosis coding errors in claims data, only patients who underwent active treatments were included. Thus, after excluding patients with C61 code at 2002 (n = 95) and those who did not have claims data of active treatments for PC (n = 2,365), a total of 873 patients who had received active treatments for newly diagnosed PC constitute the study population.
Treatment methods were classified based on primary treatment modality which includes radical surgery, RT and ADT. Surgery includes open/laparoscopic radical prostatectomy (KNHI reimbursement code ‘R3950’ and ‘R3960’) and robot-assisted radical prostatectomy. Because robot-assisted radical prostatectomy is not reimbursed by KNHI and unidentifiable by treatment codes, we operationally defined it as the absence of surgery code despite the presence of general anesthesia (code ‘L1211’) and postoperative pathologic examination code (code ‘C5500’ or ‘C5504’ or ‘C5505’ or ‘C5508’ or ‘C5918’ or ‘C5919’), as described in our prior study (20). RT includes all types of RT including conformal and intensity-modulated RT, while primary ADT includes both surgical and medical castration. Although patients underwent additional (neoadjuvant, adjuvant and salvage) therapy before and after surgery and RT, patients were categorized in terms of their primary treatment modality (20).
Variables and statistical analysis
KNHI data includes death outcomes including cause and time. Cause of death was categorized into PC, other cancer (OC), cardiovascular disease (CVD), and other causes. OC-specific mortality indicates death due to double primary cancers that are diagnosed before or after PC. CVD mortality was defined as death due to ischemic heart disease, and/or ischemic stroke.
Potential confounders included age, comorbidity, income class, and residential area. Patient age at diagnosis was divided into four categories (< 49, 50–64, 65–74, and ≥ 75 years) (21). Information on individual comorbid conditions was aggregated with the use of the Charlson Comorbidity Index (CCI) (13). CCI scores were initially categorized as 0, 1, 2, and 3 or more, and we dichotomized CCI as present (score ≥ 1) versus absent in multivariate analyses (13). Income class was divided into 5 categories, as provided by KNHI. Residential area was divided into three categories (metropolitan, urban, suburban/rural) based on population density.
Descriptive statistics was used to characterize cause of death according to treatment modalities. χ2 tests were used to describe the relationship between the categorical variables. Kaplan-Meier survival curves were constructed to estimate overall and PC-specific mortality stratified by primary treatment modality. The log-rank test was used to evaluate the significance of survival differences. Multivariable logistic regression analysis was used to determine the adjusted odds ratios (OR) and 95% confidence intervals (CI) of sociodemographic factors as well as primary treatment modality that were significantly associated PC-specific death. Annual P for trend for each cause of death was determined by Wilcoxon-type test for trend across ordered groups. All tests were two-tailed, with P < 0.05 considered significant. Statistical analysis was performed using Stata/SE software, version 12.1 (Stata Corporation, College Station, TX, USA).
RESULTS
Characteristics of the study population
Table 1 summarizes the patient characteristics. Patients undergoing surgery, RT, and ADT constituted 36.9%, 13.2%, and 49.9%, respectively, of the study population. Mean age at diagnosis was 65.7 years (SD, 9.2 years). Among entire patients, 270 (30.9%) had no comorbidity. There were 122 patients (14.0%) in the lowest income class (class 0–2), and the greatest percentage (40.7%) was in the highest income level (class 9–10). About one fourth of patients lived in a metropolitan, and over 50% of patients lived suburban or rural area. There exist significant differences in age, CCI and residential area according to the primary treatment method (Table 1).
Table 1
Characteristics of study population

Cause of death in Korean PC patients
During a median follow-up of 4.75 (interquartile range, 2.99–6.51 years), 29.4% (257/873) of the study population died. Among patients undergoing surgery, RT and ADT, 7.8% (25/322), 54.8% (63/115) and 38.8% (169/436) died, respectively. Among the 257 deaths observed in the entire cohort, PC, OC, CVD, and other causes were responsible for 46.3% (119), 35.4% (91), 6.6% (17), and 11.7% (30), respectively (Fig. 1). Significant differences in the causes of death were observed among treatment groups (Fig. 1, P
< 0.001). Only minor proportions of patients undergoing surgery and RT died from PC (20.0% of surgery and 9.5% of RT group, respectively), whereas 63.9% of ADT group died from PC. Of note, 56% of surgery group and 74.6% of RT group died from OC, while 17.8% of ADT group died from OC. Common OCs included lung, colorectal, stomach, liver and bladder cancers, although it slightly differed depending on primary treatment modality (Table 2). Among 91 patients dying of OCs, 58 (63.7%) died of OCs before PC diagnosis, and 33 (36.3%) died of subsequent OCs. CVD was responsible for 4.0%, 6.3%, and 7.1% of the causes of death in the surgery, RT, and ADT group, respectively (Fig. 1).

Table 2
Common cancers of cancer mortality other than prostate cancer

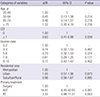
On multivariable logistic regression analysis (Table 3), a positive CCI score was associated with 37% lower odds for PC-specific mortality (adjusted OR = 0.63; 95% CI = 0.41–0.98), while ADT (compared to surgery) were associated with significantly increased odds for PC-specific mortality (adjusted OR = 16.47; 95% CI = 6.45–42.03).
Table 3
Multivariable logistic regression analysis for predicting prostate cancer-specific mortality
Overall and PC-specific survival stratified by primary treatment modalities
Five-year overall and PC-specific survival rates were 46.2% and 85.3%, respectively. Survival curves according to primary treatment modalities are shown in Fig. 2. Overall survival rates were the highest in the surgery group, followed by ADT group (Fig. 2A), while it was the lowest in the RT group (5-year survival rates: surgery, RT, ADT; 94.7%, 49.5%, and 65.8%, respectively, P < 0.001). In contrast, PC-specific survival rates were similar between surgery and RT group (P > 0.05), while it was significantly lower in the ADT group (Fig. 2B; 5-year survival rates: 98.4%, 94.1%, and 73.8%, respectively, P < 0.001).

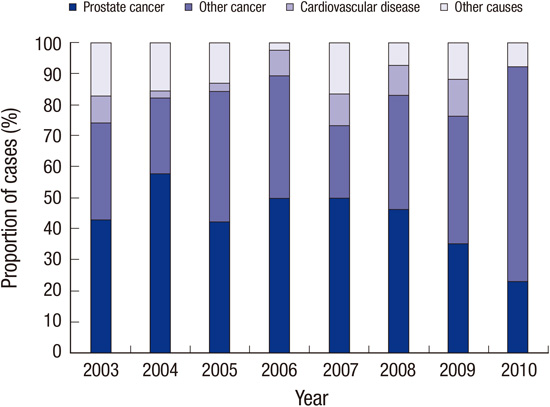
Time trends in cause of death
There have been variations in the causes of death from 2003 to 2010 (Fig. 3). The proportion of PC deaths decreased from 42.9% in 2003 to 23.1% in 2010 (P for trend < 0.001), whereas the proportion of non-PC deaths tended to increase over the 8 years (P for trend < 0.001).

DISCUSSION
To our knowledge, this study is the first one that represents competing causes of death and time trends in Korean PC patients. Given that PC tends to affect older men and prevalence of comorbidity increases with advancing age, competing causes of death are important contributors to death of PC patients (1314). We found that overall 46.3% of Korean PC patients died of PC, indicating that more than one half of the deaths are due to non-PC causes (Fig. 1). We also found that causes of death were significantly different according to primary treatment modality. A majority of patients undergoing definite therapy (80.0% of surgery and 90.5% of RT group) died from non-PC causes, whereas 63.9% of ADT group died from PC. This finding is probably attributable to difference between curative cancer control and palliation depending on the treatment modalities. PC-specific death rate in Korean population (46.3%) is relatively higher than those of US population based studies ranging from 36% to 41%, which included populations during the 1980s to 1990s (1318). This finding may reflect that significant proportions of Korean patients are still diagnosed with higher stage or grade PC than western patients, although recent increase of PSA screening in Korea contributes to stage migration toward a lower stage and grade of PC (22).
Another interesting finding is that a significant proportion (35.4%, 91/257) of decedents died of OC. Among the patients dying of OCs, about two thirds (63.7%, 58/91) died of prior OCs before PC, and about one third (36.3%, 33/91) died of secondary primary OC after PC. Among patients undergoing surgery and RT, OCs were the most common causes of death, accounting for 56% and 74.6%, respectively. Secondary cancer is more common in cancer survivors compared to the general population (23). A US-population based study showed that PC survivors are at differential relative risk for developing secondary cancer depending on cancer types (11). We found that lung, colorectal, stomach, liver and bladder cancer are common (accounting for 64.8%) causes of OC-specific death in Korean PC patients (Table 2). Of note, patients undergoing RT were responsible for more than half (51.6%, 47/91) of all OC-specific death (Table 2). Given that RT is an effective local treatment modality for clinically localized PC (2425) and PC-specific survival rates in our study cohort were comparable between surgery and RT group (Fig. 2B), this finding indicates that patients who had OC before or after PC tended to undergo RT. Considering that 12.8% (33/257 deaths) of Korean PC decedents died of subsequent secondary primary OC, clinicians should keep in mind that regular surveillance for the development of OC is crucial in follow-up protocol.
We found that the proportion of PC decedents due to CVD (6.6%) was much lesser than that of a US population based study (30.4%) (18). This finding seems to represent much lower overall prevalence of CVD in Korean PC population compared to western population. Existing evidences have shown that ADT is significantly associated with higher risk for CVD (8910). Similarly, we observed a tendency for more common CVD mortality in patients undergoing primary ADT and RT, which is frequently performed with combined ADT, compared with patients on surgery (Fig. 1).
Our results also show that presence of comorbidity and primary treatment methods independently affect the causes of death in PC patients (Table 3). As expected, patients with comorbidity were significantly associated with non-PC mortality, whereas patients undergoing ADT were significantly associated with PC-specific mortality compared to those undergoing surgery.
During the study period, the proportion of PC deaths decreased from 42.9% in 2003 to 23.1% in 2010, whereas the proportion of non-PC deaths increased (Fig. 3). This finding indicates that the majority of Korean PC patients die from non-PC causes since mid-2000s. We think that these time trends in the competing causes of death are related to earlier detection of PC. Recent increase in PSA screening and subsequent increase in early stage PC might increase the number of Korean PC patients dying of non-PC causes. Because overtreatment is a major concern in PC (2627), many studies based on western populations have presented the likelihoods of death due to competing causes and algorithms that quantified survival of patients with PC (13151617). Further studies regarding survival of Korean PC patients according to cancer stage and competing causes of death will be beneficial to shared treatment decision making between clinicians and Korean PC patients.
We acknowledge several limitations of our study. Because data regarding clinical and pathologic stage are not available in KNHI database, analysis adjusting stage could not be performed. In addition, because our study is an observational study, there were differences in baseline characteristics. Caution is needed in the interpretation of our descriptive data including survival analysis. Relative short follow-up period (median 4.75 years) is another limitation. Countering the possible limitations, our results are based on a nationwide, randomly selected population based cohort, thus generalizable to the entire Korean PC population. We also demonstrated time trends in competing causes of death in Korean PC patients over 8 years from a longitudinal database.
In summary, more than one half of deaths in Korean PC patients are due to non-PC causes, while significant differences exist in the causes of death according to treatment modalities. Overall non-PC causes of mortality increased in Korea over 8 years, although PC-specific mortality is still higher than that of US population based studies. Our results will be valuable in overviewing causes of death and time trends in Korean PC patients, and planning future health policy for PC.
 XML Download
XML Download