

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Recently, the survival rate of high risk infants, especially premature infants has increased due to the use of antenatal steroids, pulmonary surfactant treatment, and development of perinatal health care such as respiratory and nutritional management (1234). Even in Korea, the survival rate of very-low-birth-weight infants (VLBWI) has been reported to be constantly increasing in the past half century (567). However, the crude birth rate is decreasing in Korea and the level of decrease became even greater in the past years, with 1.19 per 1,000 fertile women of total fertility rate in 2013, marking the lowest in the world (8). At the same time, births of low birth weight infants, premature infants, and multiple births are increasing due to the increase of maternal age from late marriage and development of assisted reproductive technology (910). In fact, VLBWI whose birth weight is lower than 1,500 g or extremely low birth weight infants (ELBWI) whose birth weight is lower than 1,000 g require professional and intensive care after birth in many cases, and still have high mortality and morbidity despite such treatments (1112). If they do not receive proper treatment, it negatively affects them, their families, and their countries economically and mentally for the rest of their lives, and the relevant social costs also increase later on. Therefore, improvement of their treatment outcomes is an important issue that Korea faces with the era of low birth rate. Although U.S. and Japan exhibit relatively high crude birth rates compared to Korea, they have recognized the importance of intensive care for infants from early on, and are collecting data by organizing a network centered on neonatal intensive care units (NICU). By sharing network data obtained from such processes, they are attempting to achieve quality improvement (QI) (131415). Also in Korea, the Korean Society of Neonatology along with Korea Center for Diseases Control and Prevention established the Korean Neonatal Network (KNN) database based on the web-based registration system for VLBWI, among those receiving inpatient treatment in NICUs, in order to improve the survival rate of high risk infants and reduce major complications (16).
Therefore, we aimed to examine the current survival rate of VLBWI in Korea during the hospitalization in the NICU according to birth weight and gestational age, investigate the changes in the survival rate of VLBWI and ELBWI previously reported in Korea, and compare the VLBWI survival rate of Korea with those from the networks of Japan, U.S., Canada, Australia-New Zealand, and European countries.
MATERIALS AND METHODS
Data collection
In this study, in order to obtain the current survival rate of VLBWI in Korea based on the KNN database, data were obtained from medical records of 2,386 VLBWIs who were born or transferred within 28 days from birth to 55 medical institutes participating in the KNN study with an agreement to KNN registration and received treatment during the hospitalization at a NICU from January 2013 to June 2014. In order to reduce skew of mortality, the unregistered data of 220 patients who were admitted to a NICU participating in the KNN study with only birth weight, gestational age, and cause of death before discharge known due to parent refusal, were added after the approval of institutional review board, and a total of 2,606 VLBWIs were selected. Infants who were stillborn or died before admission to NICUs after birth were excluded from this study.
To examine the trend in survival rate of VLBWI in Korea, data from 43 survival rate report analyses covering the years 1959 to 2011 (1718) were used as the basis and then data were added from subsequent nationwide investigations (567) and the current KNN study. The data were classified based on a time window on a time according to the birth year and birth weight. Then, the numbers of survival and mortality in VLBWI and ELBWI were examined and were retrospectively and comparatively analyzed (19). In addition, in order to accurately assess the trend of survival rate changes in the recent 10 yr, data on NICU survival rates previously published in 2002 (10,814 cases), 2007 (8,739 cases), and 2009 (11,864 cases), when nationwide investigations of NICU survival rates were conducted, were conducted (567), were compared with KNN data (2,606 cases) obtained from this study.
To compare the survival rate of VLBWIs between Korea and other countries, recent annual reports of the national neonatal networks of Japan, Canada, Australia-New Zealand, and European countries were used: Neonatal Research Network of Japan (NRNJ, 2012, 5,214 cases) (20), Canadian Neonatal Network (CNN, 2013, 2,876 cases) (21), Australia-New Zealand Neonatal Network (ANZNN, 2012, 2,981 cases) (22) and European Neonatal Network (EuroNeoNet, 2012, 5,103 cases) (23). In the cases of the U.S., data published in 2009 from Vermont Oxford Network (VON, birth weight 501-1,500 g) for birth weight (11), and data published in 2008-2011 from National Institute of Child Health and Human Development Neonatal Research Network (NICHD, gestational age 22-28 weeks) for gestational age were cited and presented (1). Birth weight and gestational age reported from each country were comparatively analyzed with Korea's KNN data for each section of birth weight and gestational age (Fig. 1).
Data analysis
For the survival rate trend of VLBWIs and ELBWIs in Korea, the total number of survivors in VLBWIs and ELBWIs and the total number of subjects were evenly distributed for each year according to study period for the data collected from each of the 46 previously published reports. Here, KNN data from 2013 to June 2014 were added, and the classified data were organized with time parameters with 5 yr intervals for presentation of the results. Thereby analyzed survival rate trend for each year with 5 yr interval was presented, and the year which showed a statistically significant difference in the survival rate compared to that from late 1960s was obtained. Regression analysis was performed for data from recent 10 yr when nationwide investigation on treatment outcomes was conducted, and after evaluating whether effects of the birth year and the gestational weeks and their correlation were significant, survival rates for each gestational age according to year was compared. Moreover, in order to verify which gestation periods showed improved survival rates based on birth year, the differences in the survival rates between adjacent gestation periods (e.g.; 23 weeks vs. 24 weeks, 24 weeks vs. 25 weeks) within the same birth year were compared. For the comparative analysis between countries, survival rate according to birth weight and gestational age addressed in the annual report of each country's network were compared with KNN data, and after evaluating whether the differences between countries, statistical differences in each gestational age and birth weight were compared to the KNN reference. In the case of the U.S., as data on the number of survivals and the total number could not be obtained, survival rate was presented but statistical comparison could not be performed.
Statistical analysis
For group comparisons of survival rate from various sources of summary data, generalized estimating equation (GEE) was conducted to incorporate dependent structures of available data, which were correlated within measurement periods. As well, unlike the comparison of the independent experimental group and the control group, survival rate data according to certain period or birth weight/gestational age of each country are repeatedly-measured data and thereby show within-subject correlation (24). If such a dependent structure within subjects are ignored and the test is performed for each time point or section to compare the means between the groups, information of changes within subjects are lost and the tests of multiple time points are performed repeatedly, thereby causing the problem of multiple comparison in which type I error increases. Therefore in this study, the survival rate of each group was compared using a generalized estimating equation, which is a regression analysis method for categorical outcomes considering within-subject correlation (25), and examined whether there were differences in the survival rate based on birth year, birth weight, and gestational in Korea, and further analyzed the difference in the survival rates based on birth weight and gestational age between different countries. P value <0.05 was defined as statistical significance, and significance was adjusted with the number of tests when a multiple test was needed. Statistical analyses were performed using SAS (version 9.4, SAS Institute, Cary, NC) program.
RESULTS
Current survival rate of VLBWI in Korea, 2013-2014. 6.
According to KNN data, the survival rate of VLBWI in Korea from January 2013 to June 2014 based on the point of discharge from the NICU was 84.8% (88.1% in KNN registered, 49.1% in un-registered), and the survival rate of ELBWI was 69.6% (76.3% in KNN registered, 19.8% in un-registered). When classified according to the gestational age, the survival rate was 13.8% at 22 weeks, 59.6% at 24 weeks, 70.4% at 25 weeks, and over 90% after 29 weeks (Table 1). The survival rate was higher as birth weight and gestational age increased, and more than two-thirds of the premature infants survived whose birth weight was higher than 700g and gestational age more than 25 weeks.
Changes of survival rate of VLBWI and ELBWI in Korea from 1960s to now
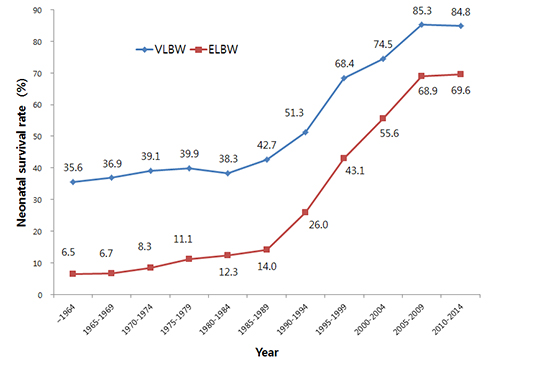
The survival rate of premature infants in Korea according to time showed a constant increase as shown in Fig. 2. From the analysis period from 1959 to June 2014 with 5 yr intervals, the VLBWI survival rate showed an increase up to 84.8% recently after a rapid increase from 35.6% in the early 1960s to 51.3% in the early 1990s. The ELBWI survival rate showed even more rapid improvement at 69.6% recently after a gradual increase from 6.5% in the 1960s to 26% in the early 1990s, showing marked improvement of survival rate within the same period compared to VLBWI. When a statistical difference in the survival rate according to each period with 5 yr intervals was analyzed based on the survival rate of the 1960s, in the early stage of the study, both VLBWI and EBLWI showed significantly rapid improvement of survival rate from the early 1990s (P=0.05 for VLBWI, P=0.013 for ELBWI).
Changes of recent survival rate of VLBWI and ELBWI from nationwide investigation
Three sets of data from 2002, 2007, and 2009, when nationwide investigation of VLBWI survival rate against total NICUs was conducted in Korea, and recent survival data of premature infants obtained from January 2013 to June 2014 through KNN data were classified according to gestational age to compare the changes of recent survival rate. Generalized estimating equation analysis of repeatedly measured data for gestational age according to time showed a significant difference in the corresponding year and gestational age (P<0.001), and significant interaction between the year and gestational age (P<0.026). Because such interaction indicates changes of survival rate in each gestational age according to time parameters, multiple comparisons of survival rates in each gestational stage according to each year was performed. When type I error was adjusted with the number of tests and compared, survival rate of premature infants with gestational age lower than 29 weeks in 2002, when the annual nationwide investigation first began, was lower than the survival rates of three investigated later (P<0.002). There were no differences in the survival rate in each gestational age in 2007, 2009, and between 2013 to June 2014 (Fig. 3). When the survival rate was compared among years by paring with the contiguous gestational age of the corresponding year, difference in the survival rate according to gestational age was statistically significant between contiguous gestational ages under 30 weeks in 2002, under 29 weeks in 2007, under 28 weeks in 2009, and under 27 weeks from 2013 to June 2014, and this shows that improvement in the survival rate was observed at younger gestational age over time (Table 2).
Comparison of recent VLBWI and ELBWI survival rates between countries
When the difference of survival rates in each country was compared according to birth weight, total survival rates of VLBWI were 93.8% (4,892/5,214), 90.2% (2,593/2,872), 92.2% (2,749/2,981) and 89.4% (4,562/5,103) in Japan, Canada, Australia-New Zealand, and European countries, respectively, which were higher than 84.8% of Korea. Their survival rates of ELBWI were also higher than that of Korea (Japan 89.4%, Canada 79.6%, Australia-New Zealand 83.3%, and European countries 78.2% vs. Korea 69.6%, Fig. 4). When the survival rates were compared according to each section of birth weight, survival rates of 500-1,000 g in Australia-New Zealand and Europe were higher than that of Korea, but there was no difference in the survival rate for groups below 500 g and over 1,000 g. Survival rates in all sections of birth weight lower than 1,200 g in Japan and lower than 1,250 g in Canada were higher than that of Korea, and especially in Japan, survival rates in all sections with birth weight below 1,000 g were markedly higher than that of Korea (Table 3). However, when survival rates of these countries and Korea were compared according to gestational age, it showed a different trend from the differences in the survival rate according to birth weight. In all countries except for Japan, differences in the survival rate with that of Korea decreased. Survival rates for 23 weeks and less, which is considered as a week for limited survival in most countries, showed no difference between Korea and all countries except for Japan. Most countries including Korea showed 60%-70% survival rate for 24-25 weeks while Japan showed a more than 80% survival rate. The survival rate of Japan showed a tendency to be maintained higher than the survival rates of other countries according to gestational age up to 28 weeks (Table 4).
DISCUSSION
According to our current KNN study, the latest VLBWI and ELBWI survival rates until NICU discharge in South Korea were 84.8% and 69.6%, respectively, indicating clear improvements (approximately two- and ten-fold, respectively) over the past half century. These improved premature infant survival rates from Korea are approaching those of the United States, Canada, Australia, and the European Union but are still far from those of Japan, which exhibits best-in-the-world treatment outcomes. In Korea, where modernized premature infant treatments started later than in other countries, there has been a pattern of low survival rates from the 1960s and gradually increasing until the 1980s, then showing dramatic increase in the 1990s that continued until the late 2000s and plateauing in the 2010s. These results are similar to those of a previous study by Kim et al. (17), who reported that improvements in survival rates of premature infants in Korea were dramatic during the early 1990s, and studies from the United States and Canada reporting that continued improvements in VLBWI survival rates were no longer seen after the 2000s (3426). Actually, confirming the age-based survival rates according to previously published reports without collecting continuous treatment outcome data can create a significant amount of errors (31314272829). Particularly in Korea, nationwide surveys on premature infant survival rates prior to the 2000s did not exist, and mostly treatment outcomes from single institutes (including four multi-center studies) of varying sizes and levels had been reported with some overlapping survey periods. Previous papers on survival rate trends simply divided the total number and the survival number of VLBWI and ELBWI reported by each institute into five-year intervals and compared them narratively (1730). However, this method can created problems of having overlapping durations between individual studies and ignoring effect size. The present study used the number of premature infant participants and survivors reported in the study by Kim et al. (17) as the basis and added data from reports published thereafter (56718) and the current KNN study for our analysis. The number of participants and survivors between each study was divided into the study duration and evenly distributed to the corresponding study year. The data evenly distributed by each year were summed according to sequential year order from 1960 to 2014, spanning the entire survey period for considering the effect size (19). Then, the data were organized by time variables of five-year increments, resolving the above mentioned problems and enabling more accurate statistical analysis. The dramatic increases in survival rates in the early 1990s in Korea that were analyzed in this manner were consistent with the timing of when Korea first began using surfactants while the number of hospitals with neonatal intensive care units equipped with incubators and artificial ventilators slowly increased (31). It is believed that the establishment of the Korean Society of Neonatology, the Korean government's expansion of support programs for premature infants, the emergence of large level III units as in developed countries, and nation-wide expansion of systematic education of neonatal cardiopulmonary resuscitation played significant roles in the dramatic increases in survival rates from the 1990s to today (31).
We confirmed that improvements in survival rates at gestational age below 29 weeks were mainly made in 2007 by performing multiple comparisons by year on three nation-wide surveys on premature infant survival rates performed in the most recent 10 yr and the survival rates per gestational age from this KNN study. Moreover, GEE statistics revealed a statistical significance in the corresponding year and gestational age, and significant interaction between the year and gestational age (Fig. 3). As a result of confirming the gestational age (statistical differences between adjacent gestational ages) in which survival rates improved for each survey year, improved survival rates were found in gestational ages of 30 weeks in 2002, 29 weeks in 2007, 28 weeks in 2009, and 27 weeks in 2013-June 2014, suggesting that survival rates in extremely premature infants are continuing to show increases in Korea, albeit slowly. This finding was in accord with the study by Kusuda et al., who reported that mortality rates for gestational age 28 weeks or higher were already sufficiently reduced and that more efforts should be made in the future for survival of smaller and more premature infants with threshold viability (32). The same study reported that survival rates of premature infants with marginal viability increased between 2003 and 2008 in Japan through a constant attitude of resuscitation. It can be inferred from the increases in the numbers and rates of registered premature infants under 28 weeks in the three nationwide retrospective studies and within the study period of the current KNN study that aggressive treatment of younger and smaller infants is also being attempted in Korea, just as in Japan (Table 2).
Although most countries have reported recent improvements in premature infant survival rates (1234), there are still discrepancies in the survival rates between the countries, which appear prominently between developed and developing countries but also exist among developed countries (13141532333435). Therefore, comparing the differences in premature infant survival rates between countries and analyzing the possible causes are very meaningful and significant. However, the presence of confounding factors must be considered when comparing survival rates between countries or regions (2728). These confounding factors include not only the biomedical domains like premature infant enrollment rate and inclusion criteria but also social domains, such as racial, economic, and political differences (37). In order to reduce these confounding factors, the current 2013-June 2014 KNN study prospectively collected data by matching the inclusion/exclusion criteria from other countries' networks as much as possible (20212223). Moreover, in order to reduce the distortion in the mortality rates, analysis included de-identified data of 220 VLBWI patients who received in-hospital treatments in the KNN participating NICU but whose guardians did not consent to participation in the study (early death was the most common reason for the non-consent, because of which the survival rates of these 220 VLBWI patients was low at 49.1% while ELBWI was 19.8%). In the present study, the survival rates of VLBWI and ELBWI in Korea were marginally lower than in most countries with which statistical comparison was possible, with the exception of the United States. Further comparisons by dividing them into more detailed birth weight groups showed that these differences can be attributed to survival rates of smaller infants below 1,000 g. However, it was discovered that comparing the survival rates between countries based on gestational age showed reduced differences in the survival rates, with the exception of Japan. Analysis of survival rates by gestational age compares birth weight-specific data to reduce the skewing caused by more mature infants based on growth restriction and is known to have the advantage of providing the doctors and parents with appropriate information before measuring the weight prior to birth (2333). As found from this comparison of the survival rate through the network data of developed countries, the reduced difference in the survival rate according to gestational age compared to that according to birth weight, but it was not analyzed in this study due to limited data whether it was because Korea had fewer cases of small for gestational age infants that had lower birth weight but somewhat more matured or because statistical power dropped due to division into smaller segments than that for birth weight. However, considering the fact that current comparative studies on premature infant survival rates regard gestational age to be more important than birth weight (3336), the small differences in survival rates based on gestation between countries appeared to be a more favorable outcome. In the present study, statistical comparison with the United States was not possible since only the survival rates and not the number of registered infants for both birth weight and gestational age were used, but the overall survival rate was low. However, Rossen et al.'s report (38) that there was a major difference in survival rates between Caucasians and African Americans stemming from socioeconomic and racial differences points out the need for future comparisons of racial and socioeconomic differences with more detailed network data. Another interesting fact not listed in the table is that, among VLBWI, the rate of gestational age below 25 weeks was higher in Japan and Korea than in Canada and Australia. According to international comparative studies after 2000, treatment approaches for extremely premature infants can be divided into comfort (palliative) and active (intensive) care (36). The studies also reported that attempting active management on those exhibiting marginal viability resulted in increased survival rates and reduced the complication rates in infants with higher gestational ages, and continuing such effort also increased the survival rates of lower gestational ages (236). Considering that Japan, an exemplary country that has implemented active care for extremely premature infants, actually has the best treatment outcomes in the world, the fact that the rate of extreme premature infants being treated in Korea is high is an encouraging sign for future improvements of their survival rates. Moreover, in the case of Japan with the highest survival rate of premature infants in international comparative studies, all-out governmental support has been reported with government-supported special care for premature infants starting from 1958 followed by implementation of government support and localization of perinatal care in 1979. Moreover, a maternal-fetal ICU started operating by 1984 and it was expanded to tertiary central perinatal care centers and secondary regional perinatal care centers; moreover, and from 1996 onwards, networks were combined for each prefecture (33). As of 2012, when an annual report was published, there were 92 tertiary central perinatal care centers and 284 regional perinatal care centers (20), and the outstanding perinatal care system that covers the entire country is believed to be related to maintaining good treatment outcomes.
There are some limitations in the present study. First, since it was a retrospective study using published reports that did not include current survival rates in Korea (KNN 2013-June 2014), there may be several confounding factors. In particular, since the survival rates prior to 2000 came from individual institutes that were large hospitals with good treatment outcomes, it is possible that the national survival rates at the time could have been lower than reported. Moreover, because "pre-viable" was not defined, data on stillbirth and miscarriage from each country were missing, and there were differences in the criteria for applying resuscitation during child delivery. Furthermore, the present study did not compare morbidity even though a report on quality improvement of neonatal care indicated that treatment outcomes should be accompanied by investigations on complications or morbidity since improved survival rates in extreme premature infants can lead to increased medical costs due to increased morbidity (23639). However, Japan, which exhibits the best-in-the-world premature infant treatment outcomes despite having a low birth rate similar to that in Korea, has been able to maintain its current low levels of neurological complications such as intraventricular hemorrhage and periventricular leukomalacia, by regularly performing resuscitation and treating premature infants between gestational ages of 22 and 24 weeks, this provides us with significant implications (1540).
Korea now has its own neonatal network that accumulates and provides accurate data on premature infants representative on a national level, similar to the Vermont Oxford Network or NICHD in the United States, Neonatal Research Network in Japan, and Canadian Neonatal Network in Canada. This network made possible investigation of survival rates as well as short- and long-term complications in premature infants. Furthermore, it was confirmed through the current KNN data (along with previously published data) that the survival rates of premature infants in Korea is continuing to increase and getting close to those from other developed countries. Moving forward, efforts will be necessary to continue accumulation of data through the Korean network and to share and analyze the data obtained with data from networks of other developed countries so that better treatment approaches can be chosen and quality improvements can be made to bring treatment outcomes in premature infants a step higher.




 XML Download
XML Download