

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Recently, the incidence of fungal endophthalmitis has increased, particularly in developing countries (1, 2, 3, 4). Fungal endophthalmitis is a serious ocular condition associated with potentially devastating visual outcomes, which originates from either direct inoculation of a fungal organism or hematogenous dissemination (5, 6). Direct inoculation of a fungal organism (exogenous endophthalmitis) can be caused by trauma or intraocular surgery (e.g., filtering surgery or phacoemulsification), whereas hematogenous spreading (endogenous endophthalmitis) can be caused by systemic fungal infection. Most patients with endogenous fungal endophthalmitis have predisposing systemic risk factors, such as systemic debilitating disease, an immunocompromised status, recent hospitalization, diabetes, malignancy, central lines, systemic surgery, organ transplantation, liver disease, renal failure, intravenous drug use, or parenteral nutrition (7, 8, 9). By contrast, exogenous fungal infection usually occurs in immunocompetent patients.
The most common causative organisms of endogenous fungal endophthalmitis are Candida spp. (9, 10). For exogenous endophthalmitis, molds such as Fusarium and Aspergillus spp. are the most common causative organisms (11, 12). The causative organism of fungal endophthalmitis can differ in association with the underlying cause and immune status of the patients. Moreover, the treatment methods depend on general condition of the patient and have changed with improvements in vitreoretinal surgical techniques. Chakrabarti et al. (10) reported that the combination of pars plana vitrectomy and intravitreal amphotericin B was the most common treatment method for fungal endophthalmitis. Therefore, in this present study, we aimed to identify the causative microorganism of fungal endophthalmitis in cases who were treated at a tertiary eye center in Korea from January 2007 through October 2013. Additionally, we analyzed differences in visual prognosis according to the treatment method and route of infection.
MATERIALS AND METHODS
Study design and participants
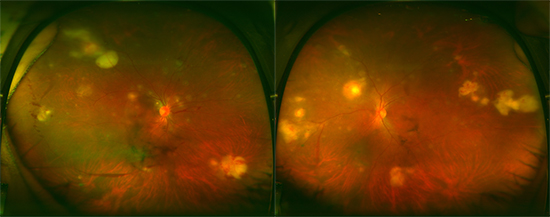
A retrospective review was conducted of all patients who were diagnosed with fungal endophthalmitis at the Asan Medical Center, Seoul, Korea, from January 2007 to October 2013. Fungal endophthalmitis was diagnosed when iritis, vitritis or yellow/white circumscribed chorioretinal infiltration on ophthalmic examination was found with one or more of the following: positive aqueous or vitreous cultures, or culture-verified systemic fungal infection. We diagnosed fungal endogenous endophthalmitis when yellow/white circumscribed lesions were found with systemic fungal infection. If patients had yellow/white circumscribed lesions with a history of trauma or recent intraocular surgery, and a microorganism was identified in the anterior chamber or vitreous fluid, we diagnosed exogenous fungal endophthalmitis.
Primary and secondary objectives
The primary objective of this study was to identify the causative micro-organism of fungal endophthalmitis. Secondary objectives included determination of the following: 1) differences in visual prognosis between endogenous and exogenous fungal endophthalmitis; 2) treatment methods for fungal endophthalmitis; 3) differences in visual prognosis according to the treatment method; and 4) systemic risk factors for endogenous endophthalmitis.
Ophthalmic examinations
All patients underwent a complete bilateral ophthalmic examination, including best-corrected visual acuity (BCVA) using the Snellen chart. BCVA results were converted to the logMAR scale. Patients who were only able to count fingers, detect hand motion, light perception, or no light perception were assigned logMAR values of 2.0, 2.3, 2.7, and 3.0, respectively (13). All patients also underwent biomicroscopic and fundus examinations.
Treatment of fungal endophthalmitis
In all cases of endogenous endophthalmitis, intravenous antifungal agents were initially administered. If vitreous involvement of a fungal pathogen, such as vitritis, iritis, or fovela involvement, was suspected, an intravitreal amphotericin (0.01 mg/0.1 mL) or intravitreal voriconazole (0.05 mg/0.1 mL) injection was administered and repeated intravitreal antifungal agent injections were administered at 1-week intervals until the clinical signs of endophthalmitis improved. If the general condition of the patient tolerated a surgical procedure, prompt vitrectomy, vitreous sampling, and intravitreal antifungal agent injection (amphotericin or voriconazole) were performed. For exogenous endophthalmitis, prompt vitrectomy and intravitreal antifungal injection (amphotericin or voriconazole) were performed. If the inflammation was too severe to preserve the eyeball, evisceration was performed.
Statistical analysis
The Kolmogorov-Smirnov test was used to determine whether data were normally distributed. Visual prognosis and the treatment method were compared between endogenous and exogenous endophthalmitis groups using the Mann-Whitney test, Pearson chi-square test, and Fisher's exact test. To analyze differences in visual prognosis between intravitreal antifungal injection and vitrectomy, the Mann-Whitney test was used. To compare pretreatment logMAR BCVAs and post-treatment log-MAR BCVAs, the Wilcoxon signed rank test was used. For all analyses, SPSS version 21.0 (SPSS, Inc., Chicago, IL, USA) was used; P values<0.05 were considered to indicate statistically significant differences.
RESULTS
Causative organism of fungal endophthalmitis
A total of 40 eyes were diagnosed with fungal endophthalmitis at the Asan Medical Center between January 2007 and October 2013.
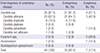
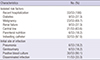
Table 1 shows the fungal species isolated from patients with fungal endophthalmitis. A total of 40 eyes from 30 patients with fungal endophthalmitis were included in this study. Among these 40 eyes, 33 and 7 eyes were endogenous and exogenous endophthalmitis, respectively. Candida spp. were the most common causative organisms in fungal endophthalmitis (35/40, 87.5%). In eyes with endogenous endophthalmitis, 91.2% (31 eyes) were infected with Candida spp., and in 1 and 2 eyes Fusarium and Scedosporium were detected, respectively. In exogenous endophthalmitis eyes, 57.1% (4 eyes) were infected with Candida spp., and in 2 and 1 eyes we detected Fusarium and Acremonium, respectively.
Visual prognosis of fungal endophthalmitis
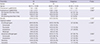
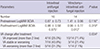
Table 2 shows the visual prognosis and treatment of cases of endogenous and exogenous fungal endophthalmitis. Pre- and post-treatment BCVA were not significantly different between the endogenous and exogenous fungal endophthalmitis groups. A total of 14 eyes were treated by vitrectomy with intravitreal and intravenous antifungal agent administration. Additionally, 16, 9, and 1 eyes were treated by intravitreal antifungal agent injection (voriconazole or amphotericin) with intravenous antifungal agent, intravenous antifungal agent alone, or evisceration, respectively. Visual prognosis according to the treatment method are shown in Table 3. Pretreatment BCVA was not significantly different between the intravitreal antifungal injection groups (intravitreal antifungal injection, 0.87±0.73; vitrectomy, 1.41±0.96; P=0.116). After vitrectomy, the logMAR BCVA significantly improved from 1.41±0.96 to 0.96±0.77 (P=0.012). However, no difference was detected in the group administered intravitreal antifungal injection alone. The proportion of eyes that gained more than a two-line visual improvement was 71% in the vitrectomy group and 25.0% in the intravitreal antifungal injection group (P=0.011). In the intravenous antifungal agent alone-treated group, visual acuity was worsened after treatment (from 0.54±0.27 to 0.92±0.65, P=0.109); however, this difference did not reach our threshold for statistical significance.
The systemic risk factors for endogenous fungal endophthalmitis are shown in Table 4. All patients had a history of recent hospitalization. There were 23 eyes (69.7%) that had an underlying malignancy and 21 eyes that had a central line. Additionally, among 23 patients with endogenous endophthalmitis, 12 (52.2%) patients died because of systemic fungal infection.
DISCUSSION
Fungal endophthalmitis is a rare ocular condition that can be caused by the hematogenous spread or direct inoculation of a fungal organism. Exogenous fungal endophthalmitis usually occurs after filtering surgery, cataract surgery, or trauma, whereas endogenous endophthalmitis develops during a systemic fungal infection. Herein, we analyzed the causative organisms for recent cases of fungal endophthalmitis and studied the visual prognosis of fungal endophthalmitis according to the route of infection and treatment method at a tertiary referral center in Korea.
A previous study reported that the most common causative organisms of endogenous fungal endophthalmitis were Candida spp. By contrast, for exogenous endophthalmitis, mold (Fusarium spp. and Aspergillus spp.) was the most common causative fungal agents. Wykoff et al. (11) reported that filamentous fungi (molds) accounted for 35 (85%) cases of exogenous endophthalmitis and that Candida species (yeasts) accounted for 6 (15%) cases. Pflugfelder et al. (12) reported that 90% of exogenous fungal endophthalmitis cases were caused by mold.
In both this present and previous studies, we found that the most common causative organisms of endogenous fungal endophthalmitis were Candida spp. However, Candida spp. were the most common causative organisms in exogenous fungal endophthalmitis, unlike previous studies, which reported that the most common causative fungal organisms were molds. Other studies reported that Candida spp. were the main mycotic causes of exogenous endophthalmitis in the postsurgical group, whereas Fusarium spp. were the main causative organisms for post-traumatic and postkeratitis patients (14, 15, 16, 17). In our present study, among 7 eyes with exogenous endophthalmitis, 6 were a result of postsurgical endophthalmitis and 1 was caused by fungal keratitis. Therefore, unlike previous studies, Candida spp. appeared to be the most common causative organisms in our current analysis (4/6, 66.7%).
We also analyzed the visual prognosis of fungal endophthalmitis based on the route of infection and method of treatment. We found that pre- and post-treatment BCVA were not significantly different according to the route of infection. Additionally, the degree of BCVA improvement was also not significantly different between different routes of infection (endogenous vs. exogenous). However, the amount of BCVA improvement was significantly different according to the treatment method. We found that BCVA significantly improved after vitrectomy, whereas BCVA did not improve after intravitreal antifungal injection. In this study, 14 and 16 eyes were treated by vitrectomy with intravitreal antifungal injection or intravitreal antifungal agent injection alone using voriconazole or amphotericin, respectively. In some patients of the intravitreal antifungal injection group, we could not perform vitrectomy because of the poor general condition of the patient. Actually, the poor general condition of these patients who could not undergo vitrectomy might have affected the poor visual prognosis of the intravitreal antifungal injection group. We considered that if the general condition of the patient permitted a surgical procedure, a combined treatment of prompt vitrectomy and intravitreal antifungal agent injection could improve visual acuity.
We also analyzed the systemic risk factors and mortality of endogenous endophthalmitis. Patients with fungal endogenous endophthalmitis usually had several systemic risk factors. Herein, all patients with endogenous endophthalmitis had a history of recent hospitalization. Additionally, 23 (69.7%) eyes were from patients who had an underlying malignancy and 21 (63.6%) eyes were from patients who had a central line. Because of several systemic risk factors, the mortality rate of endogenous fungal endophthalmitis was generally high. Menezes et al. reported that the mortality rate of endogenous Candida endophthalmitis was 77% (18). In this present study, the mortality rate of endogenous endophthalmitis was 52.2% (12/23 cases). We believe that the overall mortality rate was slightly reduced because of advances in antifungal therapeutic drugs.
Our present study had several limitations, which were inherent to its retrospective design. The sample size was also relatively small, which likely limited the statistical strength of our analysis. Additionally, some endogenous fungal endophthalmitis cases were diagnosed based on clinical features and systemic fungemia without microbiological organism identification in the vitreous or anterior chamber fluid. Therefore, future studies that examine a larger cohort of patients with culture-verified fungal endophthalmitis are needed to confirm the causes and prognosis of fungal endophthalmitis.
In conclusion, the most common causative organisms of fungal endophthalmitis were Candida species, irrespective of the route of infection. Post-treatment BCVA and the degree of BCVA improvement were not significantly different according to the route of infection. However, the amount of BCVA improvement significantly differed according to the treatment method. Moreover, we found that the BCVA significantly improved after vitrectomy, but did not improve after intravitreal antifungal injection. Therefore, if the general condition of a patient permits a surgical procedure, prompt vitrectomy combined with intravitreal antifungal agent injection can improve visual acuity.
 XML Download
XML Download