

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The survival rate of extremely premature infants, including very low birth weight infants (VLBWI), has increased due to advances in maternal fetal medicine and neonatal intensive care unit (NICU) treatment. Regardless, the incidence of bronchopulmonary dysplasia (BPD), a major cause of postnatal mortality and morbidity, has not decreased in premature infants. The risk of BPD is even higher in infants with shorter gestational periods and lower birth weights (1, 2).
Even after discharge from the NICU, there is a high rehospitalization rate in VLBWI (3, 4, 5). Respiratory syncytial virus (RSV) infection in patients with BPD is known to increase the rehospitalization rate and mortality of VLBWI, because it leads to more severe complications (6, 7, 8). According to a Korean report, 38% of VLBWI were rehospitalized within one year of discharge from the NICU, and 56% of cases were related to the respiratory system. Among these patients, 32% tested positive for RSV infection and 18% were rehospitalized within one year (9). In premature infants with BPD, the RSV hospitalization rate ranges between 8.8% (10) and 36.7% (11). RSV infection poses a risk of serious complications in premature infants, especially those with BPD. Unfortunately, an RSV vaccine has not yet been developed. However, palivizumab, a human monoclonal antibody with recombinant DNA technology, is a safe and effective (12, 13) method of preventing serious RSV disease. Palivizumab has been used in over 80 countries following its approval by the US Food and Drug Administration in 1998 (14, 15, 16, 17, 18).
Palivizumab has been marketed in Korea since 2005. It is the only preventive medication for RSV infection indicated for premature infants with BPD in Korea. However, there are few domestic reports regarding RSV infection in infants with BPD who received palivizumab prophylaxis because it has only been covered by medical insurance since January 2006. Prospective reports are lacking in regard to real-world RSV infection rates after palivizumab prophylaxis in VLBWI with BPD. There is also little information regarding differences in the RSV hospitalization rate based on BPD, and the number of administered palivizumab injections. Therefore, a multi-center, national, prospective study was conducted on RSV hospitalization rate after NICU discharge with the use of palivizumab in VLBWI with BPD. We also collected information on the following BPD risk factors: gestational age, birth weight, ventilator dependency, and the number of palivizumab injections.
MATERIALS AND METHODS
Study subjects
A multi-center, prospective, observational study was conducted to determine the rate of RSVhospitalization in VLBWI with BPD who received prophylaxis with palivizumab. Patients were prospectively recruited between September 2007 and April 2008 from the following seven tertiary care hospitals: Samsung Medical Center, Kangbuk Samsung Hospital, Cheil General Hospital & Women's Healthcare Center, Ilsan Paik Hospital, Korea University Ansan Hospital, CHA Gangnam Medical Center, and Soonchunhyang University Bucheon Hospital. The participants and their legal representatives (as children are unable to make their own medical decisions) were educated about the nature of the study and the expected results. The principal investigator obtained written consent from the subject's legal representative. No procedure or test was conducted without consent. The study subjects included former-premature children (born at 35 weeks gestation or earlier) with birth weights of ≤1,500 g, who had been treated for BPD within 6 months of the RSV season and who were ≤24 months old at the time of the study's onset. A child who required oxygen up to 28 days after birth was defined as having BPD. Subjects were excluded from the study if any of the following criteria applied: required the use of a ventilator at the start of the study, had a life expectancy of 6 months or less, had active RSV infection or a recent RSV infection, had liver or renal dysfunction, had history of seizure, immunodeficiency, or were allergic to IgG agents, received RSV immunoglobulin within three months of the study, or received any other RSV-directed monoclonal antibody or palivizumab.
Palivizumab administration
An initial dose of 15 mg/kg of palivizumab was administered to eligible study subjects. Two to five injections of palivizumab were administered monthly. In Korea, RSV season generally lasts from October to March; therefore, palivizumab administration started in September, one month before the beginning of the RSV season.
Data collection and analysis
Patient data including gestational age, birth weight, and known risk factors of RSV infection were elicited from caregiver interviews and reviews of the medical records. All assessments were conducted in person or via phone at the time of palivizumab administration. Assessments were continued for 30 days after the last palivizumab administration. Medical records related to ventilator use or the need for oxygen were reviewed as needed. The RSV rapid antigen test was performed and recorded if the subject was suspected to have been previously hospitalized with RSV.
The hospitalization rate due to lower respiratory infection with RSV after the administration of palivizumab was reviewed. Patient demographic characteristics were collected. Subjects were separated into one of three groups: the "RSV hospitalization group" (hospitalized subjects with a positive RSV rapidantigen test), the "other lower respiratory tract infection (LRTI) hospitalization group" (subjects with a medical history of hospitalization due to unknown origin or a non-RSV infection), and the "non- hospitalization group." Risk factors and the duration of hospital stays were recorded for patients with a history of palivizumab injections and RSV hospitalization.
Subjects were divided based on gestational age, birth weight, and the number of days on a ventilator. The difference in hospitalization rates due to RSV infection was investigated. The risk factors for RSV hospitalization were also analyzed for each group. Subjects were divided into the following groups based on their gestational age: <26 weeks, 26-28 weeks, and 29-31 weeks. Subjects were also divided into the following groups based upon their birth weight: <750 g, 750-999 g, 1,000-1,249 g, and 1,250-1,500 g. In order to classify the severity of the subjects' respiratory states, they were placed into the following groups based upon how long they required ventilator use: <30 days, 30-59 days, 60-89 days, and 90-120 days.
Statistical analysis
Statistical analyses sought to determine the factors related to RSV hospitalization, and were performed using SPSS version 18 (SPSS Inc., Chicago, IL, USA). SPSS was also used to analyze patient characteristics in those with RSV infection. The results are expressed as means±standard deviations. A Student t-test was used on a continuous scale, and a chi-square test was used on a nominal scale. Statistical significance was defined by P values<0.05.
RESULTS
Subject characteristics
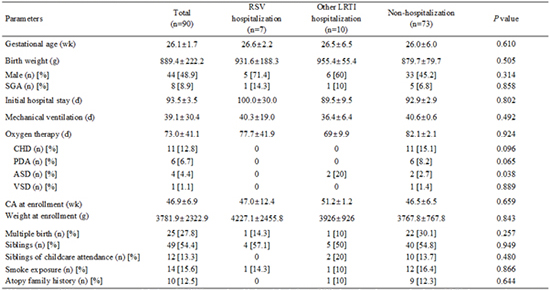
Ninety children were enrolled in the study, with 44 male (48.9%), and 46 female (51.1%) participants. The subjects' gestational ages ranged between 23 and 31 weeks (mean 26.1±1.7 weeks). Fifty-two subjects (57.8%) were 26 weeks or younger at birth. The mean birth weight was 889.4±222.2 g; 66 subjects (73.3%) weighed ≤1,000 g. All of the subjects received treatment in the NICU with a mean hospital stay of 93.5±31.1 days. Eighty-nine subjects (98.9%) were on a ventilator after birth for a mean of 39.1±30.4 days of use. All of the subjects who required ventilator support received oxygen treatment for a mean of 73.0±41.1 days. At study enrollment, the mean subject age was 46.9±15.9 weeks (ranging from 28 days to 17.8 months). The mean weight at enrollment was 3,781.9±2,322.9 g.
Analysis of the risk factors for RSV hospitalization
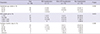
Of the 90 subjects who received palivizumab, 17 subjects were hospitalized with 21 cases of respiratory infection. A RSV rapid antigen test was conducted in 14 of the 21 respiratory cases, and eight cases of RSV were confirmed in seven subjects. Seventeen (18.9%) subjects were hospitalized secondary to their respiratory infections. And among these subjects, RSV infection was confirmed in seven (7.8%). The demographic characteristics of the RSV hospitalization group, other LRTI hospitalization group, and non-hospitalization group is presented in Table 1. The following previously reported risk factors of RSV hospitalization were not statistically associated with RSV hospitalization in our study: gestational age, weight, gender distribution, duration of hospital stay after birth, duration of ventilator and oxygen use, multifetal gestation, and the number of siblings attending preschool/elementary school.
RSV hospitalization group
Seven subjects were hospitalized with RSV infections (5 male, 2 female). One subject had two RSV infections during the observational period, making a total of eight cases. The mean gestational age of this group was 26.6±2.2 weeks (23-29 weeks); the mean birth weight was 931.6±188.3 g (652-1,185 g). The mean hospital stay length in the NICU after birth was 100.0±30.0 days (72-163 days). The mean duration of ventilator use was 40.3±19.0 days (18-77 days). The mean duration of oxygen administration was 77.7±41.9 days (35-161 days). Three subjects had a history of patent ductus arteriosus, all of which resolved prior to RSV infection. The mean postnatal ageat the time of RSVhospitalization was 199.3±93.8 days (79-312 days), and the time from hospital discharge (after birth) to RSV hospitalization was 122.6±67.6 days (32-217 days).
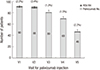
Eight cases of RSV hospitalization were observed in seven subjects. Six cases (75.0%) occurred between October and November 2007, one case (12.5%) in December 2007, and one case (12.5%) in March 2008. There were two cases (25.0%) of RSV hospitalization following one palivizumab injection, three cases (37.5%) after two injections, and one case each after three, four, and five. The incidence of RSV hospitalization based on the number of prior palivizumab injections is shown in Fig. 1. The mean number of palivizumab injections before RSV hospitalization was 2.3±1.4, which is lower than the mean number of injections received by children who were hospitalized with non-RSV infections (4.0±1.2); however, the difference was not statistically significant. The first injections were given in early September (three subjects), mid-September (one subject), late September (two subjects), and late October (one subject). The time from the last palivizumab injection to RSV hospitalization ranged from 4 to 63 days, with a mean of 21.3±16.6 days (Table 2).
The mean duration of RSV hospitalization was 11.0±5.5 days (4-18 days). There were two cases of ventilator use and oxygen treatment; among these subjects, one death occurred. The child that died was a male born at 29 weeks. His birth weight was 1,064 g, and he had received two doses of palivizumab in early September and October 2007 during his first admission. His hospitalization after birth was prolonged due to an RSV infection in mid-October. Oxygen and drug treatments with sildenafil, furosemide, and spironolactone were continued after his discharge due to severe BPD and pulmonary hypertension. By mid-January 2008, he had received five palivizumab injections. Two days after the fifth palivizumab injection, he was rehospitalized with dyspnea and decreased feeding. Although the RSV rapid antigen test was negative at the time of rehospitalization, a test in late March was positive for RSV. The patient developed worsening dyspnea and died after 7 days of pneumothorax.
Analysis of RSV hospitalization based on groups
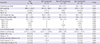
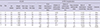
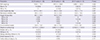
RSV hospitalization was analyzed in each of the following groups: gestational age (weeks), birth weight, and days on a ventilator (Table 3). There was a significantly higher RSV hospitalization rate in the gestational age group of 29- 31 weeks compared to that of the other gestational age groups (Fig. 2). In addition, there was a significantly higher rate of small for gestational age infants in this particular gestational age group compared to that found in other gestational age groups (Table 4). Each group was also compared with regard to gestational age, birthweight, gender distribution, duration from birth to discharge, duration of ventilator and oxygen use, multi-fetal gestation, and the number of siblings attending preschool or elementary school. There were no other significant differences between the groups, which may have been a result of the small sample sizes.
DISCUSSION
Of the 90 subjects who received palivizumab, 17 subjects were hospitalized with 21 cases of respiratory infection. Of these 21 cases, an RSV rapid antigen test was conducted in 14 cases, and eight cases of RSV infection were confirmed in seven subjects. Therefore, the overall rate of respiratory hospitalization was 23.3% (21/90), and the rate of RSV hospitalization was 8.9% (8/90). RSV accounted for 38.1% (8/21) of the respiratory infections observed. This figure may actually underestimate the true value, because one third of respiratory hospitalizations were not tested for RSV.
The rate of RSV hospitalizations in premature infants with BPD who did not receive palivizumab prophylaxis ranges from 8.8% (4) to 36.7% (5). A prior domestic study reported a rate of 22.2% (19). However, the RSV hospitalization rate after palivizumab in premature infants with BPD was found to be 5.8% (17) in the United States and 6.0% (20) in Canada. These studies included subjects at a more mature stage of development (mean gestational age of 30 weeks and mean birth weight of 1,500 g) compared to those in our study (26 weeks and 889 g, respectively). IMpact study (21) documented that after palivizumab administration in premature infants (mean gestational age of 29 weeks and mean birth weight of 1,300 g) with BPD lead to a decrease in RSV infection rate from 12.8% to 7.9%. The RSV hospitalization rate in this study (8.9%) is relatively high compared to that of other studies. However, this study included subjects who were more premature with a mean gestational age of 26 weeks and a mean birth weight of 889.4±222.2 g than were the subjects included in other studies (14, 17, 20).
Although one might hypothesize that low gestational age, low birth weight, and respiratory severity are important risk factors associated with RSV hospitalization, none of these factors was significantly associated with RSV hospitalization in our study. When the subjects were divided into three groups based on gestational age, RSV hospitalization was significantly higher in the group of subjects in the 29-31 weeks group. However, the subjects from the younger gestational age groups had longer hospital stays and spent more time on a ventilator than did those in the 29-31 weeks group. Interestingly, the proportion of small for gestational age infants was still significantly higher in the 29-31 weeks group compared to that of other groups.
At the time of RSV hospitalization, most children (5/8; 62.5%) had already received one or two injections of palivizumab. This finding is similar to the report from the Palivizumab Outcomes Registry (17) of high-risk children who received palivizumab at 35-day intervals and were hospitalized with RSV infection. They report that 75% (36/48) of RSV infections occurred prior to the third palivizumab injection. Some experts believe that three out of the five recommended administrations of palivizumab during the RSV season may be sufficient for prophylaxis. After the third palivizumab administration, the serum concentration decreases by 52% at 4 months, and by 85% at 5 months after the initial administration. After the fifth administration, however, the serum concentration is reduced to less than the fifth percentile (21). Therefore, three injections are not sufficient for complete RSV prevention. One Japanese study (22) reported that RSV can be detected in infants within 5 days of palivizumab administration, and within 20-30 days in premature infants with chronic pulmonary diseases. Palivizumab produces a prophylactic effect via passive immunity. It has a half-life of 20 days; therefore, its efficacy depends on the serum concentration that is maintained during the time of RSV exposure. Five administrations at an appropriate time interval are the most efficacious for effective prophylaxis.
RSV hospitalization occurred from September to March. Palivizumab was administered to hospitalized patients in late September (two patients) and in late October (one patient). Generally, the RSV season in Korea occurs between October and March. The incidence of infection is particularly high between November and January. Still, the RSV season varies every year, and infections can occur as early as July and as late as May (23, 24, 25). The RSV detection rate in preterm infants and LBWI are significantly higher during both the RSV season and non-RSV season compared to the rates in full-term infants (26). The incidence of RSV hospitalization in those who already received palivizumab prophylaxis may suggest that RSV exposure prior to achieving sufficient palivizumab serum concentrations may cause infection. Comorbidities like BPD in premature infants also increase the risk of infection in this group. Risk of infection is also influenced by inter-patient variability with regard to serum trough concentrations, inoculum of RSV exposure, number of palivizumab doses received and timing between the doses. It is difficult to determine the timing for optimal palivizumab prophylaxis, as the RSV season varies every year. However, the initial palivizumab administration should occur before the start of the RSV season. The RSV season in Korea (October to March of the following year) starts even earlier in high-risk, premature infants.
In conclusion, this study prospectively evaluated the incidence of RSV hospitalization after palivizumab prophylaxis in VLBWI with BPD. This is the first prospective study of palivzumab prophylaxis in a population of purely VLBWI with BPD in Korea. There are two main differences between our study andt he similar prior studies (27, 28, 29). In contrast to other groups, we conducted a prospective, observational study in formerly VLBWI with BPD, which is a very high-risk group for RSV infection. Another difference is that the subjects included in our study were younger (and smaller) than were those included in prior studies, with a mean gestational age of 26.1±1.7 weeks, and a mean birth weight of 889.4±222.2 g (14, 17, 20, 27, 28, 29). In this small group of Korean VLBWI with BPD, approximately 40% of respiratory infections were due to RSV. Even after one or two palivizumab injections, 62.5% of infants in this study still acquired RSV. With regard to this finding, it is clear that 1-2 injections are insufficient, and proper prophylaxis for high-risk children involves up to five monthly injections of palivizumab during the RSV season. Our findings can be generalized to other high-risk BPD patients who were formerly VLBWI (with similar gestational age and birth weight characteristics to those in this study) as a reference for appropriate palivizumab prophylaxis. The 29-31 weeks of gestational age group had a significantly higher RSV hospitalization rate compared to that of other groups. This particular group also had a higher rate of small for gestational age infants than did other groups. In this respect, it may be worth studying underdevelopment for gestational age.
This study has several limitations. The small sample size may have prevented detection of significant differences in the risk factor analysis. In addition, there was no control group, and the study design itself was observational, which has its own inherent limitations. However, the number of premature infants with BPD who have been injected with palivizumab is increasing, and medical insurance coverage has been expanded to children born at ≤31 weeks of gestation and less than 6 months of age at the beginning of the RSV season. Therefore, we expect that future studies will have a larger sample of infants that will more accurately reflect the epidemiology and demographic characteristics of Korea. In this manner, the most effective palivizumab administration schedule will be determined, and initiated in VLBWI to protect against RSV infection.

 XML Download
XML Download