

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Despite recent advances in medicine, attempts at improving survival rates in pancreatic cancers have failed to show any significant difference (1). Surgery is the only potentially curative treatment for pancreatic cancer, but only 10%-15% of patients are operable (2, 3). Most patients with pancreatic cancer are not candidates for surgical resection due to distant metastasis or locally advanced malignancy (4). Locally advanced malignancy refers to tumor extension that involves the adjacent organs and results in failure to achieve complete tumor free margins after surgery. In pancreatic cancer, local extension is found in about 40% of patients at the time of presentation and most commonly includes invasion of vascular structures, such as the superior mesenteric vessels or the celiac trunk (5, 6).
Interest has been increasing in preoperative treatment for pancreatic cancer, especially in locally advanced pancreatic cancer (LAPC) (7). Local treatments such as radiotherapy can attenuate the locoregional extent of the tumor. Advanced stages with vascular invasion have a higher probability of tumor micrometastasis, which can provoke early recurrence even after radical resection (8). Therefore, in these cases, systemic chemotherapy is equally important for prevention of early dissemination.
Many studies have attempted to determine the efficacy of preoperative chemoradiotherapy; however, the use of chemoradiotherapy for downstaging LAPC and conversion from an unresectable or borderline resectable state to a resectable disease remains controversial (9). Recent systematic reviews showed marginal survival benefit and little surgical downstaging in response to preoperative chemoradiotherapy in LAPC (4, 10). Nevertheless, most of the previous studies did not provide objective changes after neoadjuvant treatment (11, 12, 13, 14). In addition, some of these studies have pitfalls, as the resectability post CRRT was assessed by the response evaluation criteria in solid tumors (RECIST) without commenting on the extent of major vessel invasion (15, 16, 17).
The aim of the present study was to assess the objective changes occurring after neoadjuvant CCRT for locally advanced pancreatic cancer and to reevaluate surgical resectability after CCRT based on the extent of vascular invasion.
MATERIALS AND METHODS
Patients and clinical data
A total of 1,299 patients with pancreatic cancer from January 2003 through July 2011 were initially screened. Computed tomography (CT) indicated that 328 of these patients (25%) had suspicious major vessel invasion [superior mesenteric artery and vein (SMA/SMV), portal vein (PV), celiac artery (CA), and common hepatic artery (CHA)] without distant metastasis, which represented LAPC at the time of diagnosis. We ultimately recruited 54 patients who had pathologically confirmed pancreatic ductal adenocarcinoma and had undergone CCRT for the purpose of surgical downstaging of the tumor. The clinical data of enrolled patients were collected retrospectively based on electronic medical records.
Resectability criteria
LAPC was classified into borderline resectable or unresectable disease, based on the National Comprehensive Cancer Network (NCCN) Guidelines 2011 criteria (18). Borderline resectable disease was defined as pancreatic cancer with an abutment of the SMV/PV and of the SMA, CA, or CHA. Short-segment encasement/occlusion of the SMV/PV that allowed a safe vascular resection and reconstruction was also considered as borderline resectable. Unresectable disease was defined as pancreatic cancer with an encasement of the SMA, CA, or CHA or unreconstructible SMV/PV occlusion.
Chemotherapy and radiotherapy protocol
The CCRT regimen was based on gemcitabine, 5-fluorouracil or capecitabine with concurrent 50.4 Gy of external-beam radiotherapy given in 28 fractions. If the patients tolerated this radiotherapy, additional doses were given. The dose of each chemotherapeutic agent during CCRT was as follows: gemcitabine iv 400 mg/m2 weekly, 5-fluorouracil 500 mg/m2/day iv bolus for 3 days at 1st and 5th week, and capecitabine 800 mg/m2 per orally twice daily.
Tumor response assessment and toxicity
Resectability after CCRT was assessed by changes in vascular invasion seen by dual-phase spiral CT as well as based on the RECIST criteria. The CT images of all 54 patients were reviewed on a Picture Archiving and Communications System. CT findings regarding tumor size, major vessel invasion, and distant metastases were analyzed before and after CCRT. CT studies were assessed within 4 weeks prior to CCRT and 8 weeks after CCRT. Tumor size was measured at its longest diameter. Vessel invasion was measured by the degree of tumor contact with adjacent vasculature. Tumor involvement of vessels was graded on a scale from 0 to 4 (0 :not involved; 1:1°-90°; 2: 91°-180°; 3: 181°-270°; 4: 271°-360°) (19). Scores of 1 and 2 represented vessel abutment, and scores of 3 and 4 represented vessel encasement (20).
Toxicities during CCRT were graded by the Estern Cooperative Oncology Group (ECOG) common toxicity criteria grading system. Treatment for toxicities, including gastrointestinal symptoms, constitutional symptoms, and hematologic toxicity, were recorded.
Statistical analysis
Descriptive statistical analysis was performed using SPSS v.18.0 (IBM Corp., Armonk, NY, USA). Differences in tumor size and vessel invasion before and after CCRT were compared using a paired t-test. The relationship between chemotherapeutic agents and surgical downstaging was assessed using the chi-square test. The Kaplan-Meier method was used to analyze time-dependent variables. A P value of <0.05 was considered to be statistically significant.
RESULTS
Baseline demographics and clinical characteristics
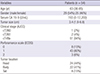
The median age of study patients was 63 yr (range 36 to 85) and there were 29 males and 25 females (Table 1). The median serum CA 19-9 level before CCRT was 193 U/mL (range 0 to 12,200). Almost all patients (51 patients, 94%) had stage III disease at baseline CT, according to the 7th edition American Joint Committee on Cancer (AJCC) Cancer Staging Manual. Of the 54 patients, 14 (26%) were found to have borderline resectable and 40 (74%) were found to have unresectable pancreatic cancers prior to CCRT, according to NCCN criteria. Invasions into the SMA, SMV, PV, CA, and CHA were detected before treatment in 38, 30, 19, 28, and 20 patients, respectively.
Objective changes in the tumor after chemoradiotherapy
The CCRT treatment consisted of administration of gemcitabine, 5-fluorouracil, and capecitabine to 17, 9, and 28 patients, respectively. The median radiation dose was 54 (range 32.4-59.4) Gy. No complete response after CCRT was observed in this study. A partial response was achieved in four patients (7%). Stable disease and progressive disease were determined in 36 (67%) and 14 patients (26%), respectively. Among the 14 patients with disease progression, four patients had local progression and the other 10 patients had distant metastasis. Tumor size showed no significant difference before and after neoadjuvant treatment (3.6±1.1 vs. 3.6±1.0 cm, P=0.61). Vascular invasion was improved in two patients (4%), while further disease progression was seen in 13 patients (24%). No significant differences were noted for PV (P>0.99), CA (P=0.53) and CHA (P=0.20) invasion following neoadjuvant treatment. SMA (P=0.008) and SMV (P=0.04) invasions were rather aggravated after neoadjuvant treatment.
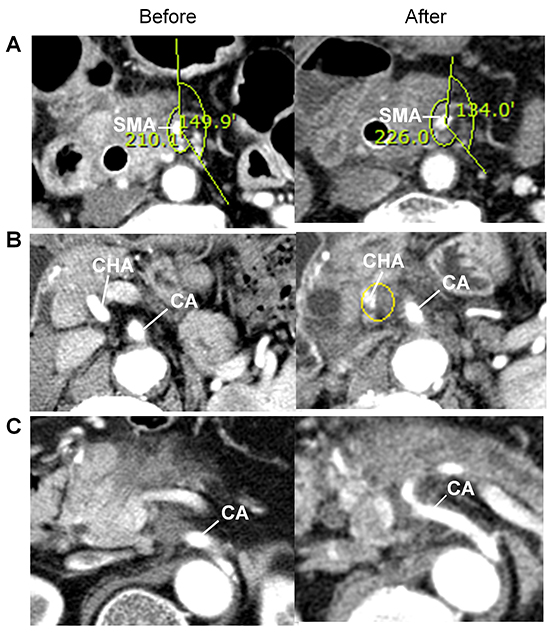
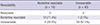
Both patients who showed vascular improvement after CCRT had unresectable disease initially: One had grade 4 CA encasement along with grade 2 CHA abutment, and the other had grade 4 CA encasement along with grade 2 CHA abutment. The first patient showed a radiologic response at CA (grade 2) and was surgically downstaged to borderline resectable disease. However, surgical resection was abandoned due to poor general condition. The second patient showed a radiologic response at CHA; however, the tumor was still unresectable as CA encasement showed no improvement. Thirty-nine patients with unresectable and 11 patients with borderline resectable pancreatic cancer at initial diagnosis still had unresectable and borderline resectable pancreatic cancers, respectively, after CCRT (Fig. 1A). Four borderline pancreatic cancers progressed further to an unresectable stage (Fig. 1B), whereas one unresectable pancreatic cancer improved to borderline resectability after CCRT (Fig. 1C). No patient improved to resectable disease staging after CCRT (Table 2). Only one patient with borderline pancreatic cancer (a 75-yr-old man with CA abutment) underwent explorative laparotomy although the radiologic response was minimal. Curative resection failed, however, due to tumor infiltration to the CA and peritoneal metastasis detected during surgery.
We investigated the relationship between chemotherapeutic agents used for CCRT and tumor progression. Tumor progression after CCRT was observed in two patients (12%) with gemcitabine, one patient (11%) with 5-fluorouracil, and one patient (4%) with capecitabine. No significant difference was seen in tumor progression after CCRT based on the choice of chemotherapeutic agent (P=0.54).
Toxicity
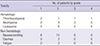
A total of 36 patients (67%) experienced CCRT-related adverse events (Table 3). The most common adverse event reported was hematology toxicity (23 patients, 43%). No CCRT-related mortality occurred. Severe toxicities (grade 3-4) arose in five patients (9%). Grade 3 toxicities developed in four patients (one developed thrombocytopenia and three developed neutropenia). One patient developed Grade 4 thrombocytopenia and treatment was withheld.
Survival analysis
During follow-up, 46 patients (85%) died and the median overall survival was 16.2 (95% CI 12.7-19.7) months (Fig. 2A). Disease progression was observed in 47 patients (87%) and the median progression-free survival was 6.4 months (95% CI 4.0-8.8) (Fig. 2B). Among the patients with disease progression, systemic presentations (36 patients, 77%) were more frequent than local progression (11 patients, 23%).
DISCUSSION
Many studies have evaluated the efficacy of neoadjuvant CCRT for LAPC; however, the ambiguous definition of the criteria for determining tumor resectability in these reports complicates judgment of the effectiveness of CCRT. Recent meta-analysis of neoadjuvant treatment in pancreatic cancer showed that the criteria for surgical resectability were either not clearly defined or not stated in more than half of the published studies (4). Our primary interest was to measure the objective changes of vascular invasion after CCRT in LAPC. Unfortunately, we found that the objective improvements of vascular invasion after neoadjuvant treatment were negligible, as none of the enrolled patients were eligible for a curative resection.
Previous studies reported various curative resection rates for pancreatic cancer after neoadjuvant treatment ranging from 1% to 71% (9, 12, 17, 20, 21, 22). The proportion of resectable, borderline resectable, and unresectable patients could significantly affect the curative resection rate after neoadjuvant treatment. In addition, the heterogeneity of radical resection rates could be explained by the different resectability criteria adopted in these studies. No patients underwent radical resections after CCRT in the present study because most patients were at an unresectable stage at the time of initial diagnosis. About 30%-40% of patients with pancreatic cancer are diagnosed as LAPC (4), but the proportion of LAPC in this study was only 25%. This showed that, at our institution, LAPC was defined when definite vascular invasion was present on CT imaging, which could have given rise to the low radical resectability rate after neoadjuvant CCRT compared to previous studies. Surgeons have different strategies for resection of pancreatic cancers and a surgeon's propensity for resection, especially in borderline resectable disease, could significantly affect the resection rate.
Surgical exploration is the most accurate method for tumor staging. One report diagnosed LAPC by intraoperative staging (either laparoscopy and/or laparotomy) (9). Of a total of 87 patients with LAPC who underwent neoadjuvant chemoradiation, only three patients had a sufficient clinical response on restaging to warrant a re-exploration. Of these three patients, only one patient had a potentially curative resection. This result is consistent with our study.
The strength of our study is that it quantitatively investigates the extent of tumor invasion in each major vessel. Some studies have assessed the effect of neoadjuvant treatment by RECIST criteria (15, 16, 17), which mainly assess the response based on tumor size and distant metastasis (23). However, the RECIST criteria do not reflect changes in vascular involvement, which is a most important determinant for the evaluation of surgical resectability. A recent study that evaluated the radiological response of patients with locally advanced pancreatic cancer found that neoadjuvant therapy did not induce radiological tumor regression (23). They evaluated the invasion of major vessels based on pre-and post-treatment CT scans. We classified vascular involvement from grade 0 to 4 and assessed the change after CCRT. These objective findings allowed accurate surgical restaging after CCRT.
The development of dual phase, thin-sectioned, and multi-detector CT imaging has improved the accuracy of preoperative staging in pancreatic cancer (24, 25, 26). However, radiotherapy causes local inflammation, resulting in over-diagnosis of vascular involvement after CCRT. This could result in misdiagnosis of patients who were candidates for surgery after CCRT as having an unresectable disease. Nevertheless, the possibility of over-diagnosis is assumed to be low, as no improvement of vascular involvement was evident on consecutive follow-up CT imaging.
As this was a retrospective study, we limited the enrollment criteria to patients with LAPC who received CCRT. This minimized the potential bias that could result from various treatments. The small number of enrolled patients precludes any recommendation that neoadjuvant CCRT should be contraindicated in pancreatic cancer. Palliative chemotherapy with FOLFIRINOX (5-fluorouracil, oxaliplatin, irinotecan, and leucovorin) has proven efficacy in metastatic pancreatic cancers (27), and FOLFIRINOX as a neoadjuvant therapy in LAPC recently showed promising results (28, 29). Future research should therefore evaluate the efficacy of preoperative treatment with FOLFIRINOX for LAPC, with a clear definition of the resectability criteria and presentation of the objective changes after therapy.
We would like to note that the present study is a hallmark study in LAPC, since the objective changes after neoadjuvant treatment were described and the surgical restaging assessment was based on these findings. The objective improvements after neoadjuvant treatment were minimal and the real efficacy of neoadjuvant chemoradiation therapy in LAPC was disappointing. Prospective studies implicating precise resectability criteria and objective changes after treatment are required to clarify conflicting results regarding the efficacy of neoadjuvant treatment for pancreatic cancer.


 XML Download
XML Download