

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Multiple myeloma, one of hematologic malignancies, is known to have a high chance of skeletal related events (SREs) from its pathologic characteristics (1, 2). Direct and/or indirect activation of osteoclast, and suppression of osteoblast proliferation are related to these SREs (3, 4, 5). Among these SREs, involvement of the spinal column predispose to pathologic fracture and neurologic complications.
In recent time, minimally invasive stabilization using bone cement has been demonstrated to be a safe and effective supportive option for spinal pathologic fractures without neurologic involvement (6, 7). Other treatment modalities such as radiotherapy, bisphosphonates and supportive treatment are also tried as adjuvant therapies (8, 9).
In our institute, each patient with this problem is addressed by a multi-disciplinary team consisting of the hematologist, radio-oncologist and spine surgeon for optimal treatment strategy. Our strategy is similar to the suggestion of Kasperk et al. (7). However, in our clinical pathway, radiotherapy is only considered in the patient with the spinal pathologic fracture and neurologic involvements by epidural myeloma. In addition, radionuclide studies have been tried for the decision of surgically augmented levels. Because most patients presented with multi-level fractures, the authors tried to select the most mechanically unstable and symptomatic levels using image studies including a radionuclide study and clinical symptoms.
This retrospective study was designed to evaluate clinical and radiologic results of bone cement augmentation procedures as an additional treatment modality for spinal pathologic fractures by multiple myeloma.
MATERIALS AND METHODS
Study population
Patients who suffered from pathological spinal fractures in conjunction with multiple myeloma were included in this retrospective study. Diagnosis of multiple myeloma was made according to the guidelines and recommendation of International Myeloma Working Group. Treatments including systemic chemotherapy, bone marrow transplantation, and general supportive therapy were mainly performed according to the guidelines of the Intenational myeloma foundation in both group patients (10, 11). During 2009-2011, 27 patients who had undergone bone cement augmentation procedures with minimum 6 months follow-up were included as the surgery group (group I). Clinical and radiological results were compared with 29 patients who had not undergone surgery, and treated conservatively as the non-surgery group (group II).
Evaluation and treatment protocol of pathologic spinal fracture
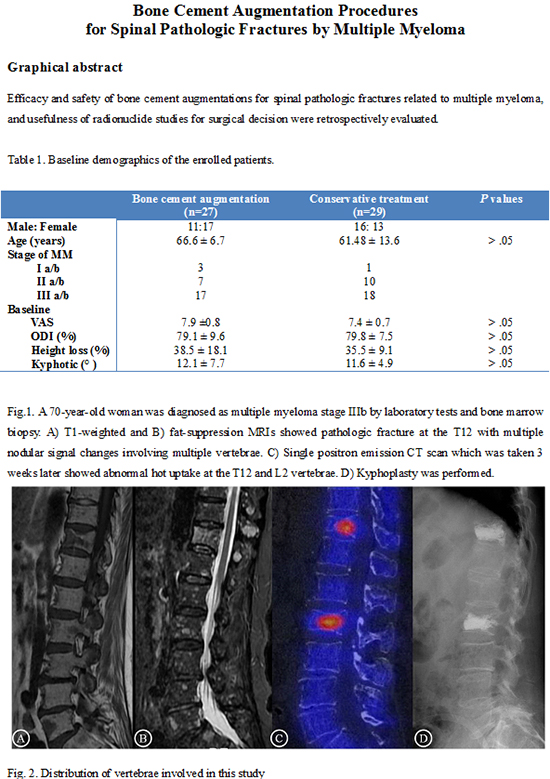
Mechanical back pain relieved by rest was the main symptom in these enrolled patients. All pathologic fractures were initially evaluated with plain radiographs and magnetic resonance images (MRIs). Involvement of posterior element or epidural extensions of myeloma were also evaluated. As candidates for bone cement augmentation procedure, unremitting back pain with visual analogue scale (VAS) ≥5 after supportive treatments were considered. For the patients who were supposed to undergo surgery, bone scan or single photon emission computed tomography (SPECT) was evaluated. The findings of these radionuclide studies were taken into account for selection of the level (Fig. 1). The location of fractured vertebrae was also considered. Mechanically demanding levels such as the thoraco-lumbar junction or lumbar level were recommended for bone cement augmentation procedures. Non-surgical treatment is more likely recommended for fractures of the mid-thoracic level. For the group II, patient's wish was one of the reasons of non-surgical treatment. General pain control and tolerable range ambulation with brace (tailor-made hard corsets) were recommended for the group II. Bisphosphonates were prescribed in all patients. Wearing of the brace was basically recommended for 3 months after initial diagnosis, and as required. For the group I, vertebroplasty or kyphoplasty was performed under local anesthesia with a mild sedation. In all surgery cases, bipedicular approach was used, and the bone cement was introduced (mean injected cement amount 4.3 mL/level). For the kyphoplasty, two balloon catheters (Kyphon®/Medtronic, Memphis, TN, USA) were used to make void, and to restore the height of the fractured vertebra. In choosing vertebroplasty or kyphoplasty, in the case of severe height loss (more than 50%) and suspicious destruction of posterior wall of the vertebral body, kyphoplasty was preferred. Postoperatively, leakage of bone cement was evaluated with postoperative CT scans.
Assessment of clinical outcomes
Basic demographics including the level of fractured vertebrae and the stage of myeloma were recorded and compared. During the follow-up periods, mortality was also evaluated. Clinical outcomes for back problem caused by pathologic spinal fractures were evaluated with VAS (0-10) and Oswestry disability index (ODI). Each parameter was questioned and recorded at baseline, 1 month and the last follow-up periods. Complications related to the surgery were evaluated.
Assessment of radiomorphological results
All radiological parameters were measured by two senior orthopedic residents who were blinded to the purpose of this study and clinical results. Height loss and local kyphotic angle of the affected vertebral body were measured using initial, postoperative 1 month and the last follow-up radiographs. Vertebral height was measured at the point of maximal collapse of the affected vertebral body and height loss (%) was calculated with a formula of ([Lower vertebral height +Upper vertebral height]/2 - affected vertebral height)/([Lower vertebral height +Upper vertebral height]/2)×100. Local kyphotic angle (°) was measured with Cobb's method between adjacent vertebrae of the affected vertebra (14). Bone cement leakage was evaluated and classified into epidural, paravertebral and discal pattern of leakage using postoperative CT scans. The ratio of the number of positive vertebrae on radionuclide scans to the number of affected vertebrae on plain radiographs and MRIs was calculated.
Statistical analysis
Data with continuance variables which included age, VAS, ODI and radiographic measurements were analyzed by t-test. Intra- and interobserver reliability for radiological parameters were assessed using Cohen's kappa statistics. Cumulative survival rate and comparison between the groups were analyzed by Kaplan-Meier analysis and log-rank test. All statistical analyses were conducted by using Statistical Product and Service Solutions (SPSS) version 13.0. A value of P<0.05 was considered to be statistically significant.
RESULTS
General demographics of both groups were summarized in Table 1. There were no significant differences in age, initial VAS and ODI, and initial height loss or kyphotic angle. Forty eight vertebrae were augmented in 27 patients of the group I. Kyphoplasty was used in 19 patients. The augmented and affected levels of each group were presented in Fig. 2. During a mean of 16.8 months (range 6-33) follow-ups of the enrolled patients, 20 patients (11 in the group I and 9 in the group II) died from complications of multiple myeloma (mainly infection including pneumonia, and cerebral vascular accident). One year follow-up cumulative survival rate were 77.4% and 74.7% in the group I and II, respectively. There was no difference in survival rate between two groups (log rank test, P=0.94). During the follow-up, other SREs besides spinal fracture had occurred in 3 patients. Subsequent fractures of the spine were noted in 10 patients (6 patients in the group I and 4 in the group II, respectively). Additional cement augmentation procedure has not been performed in all patients.
Clinical outcomes
Even though the baseline VAS and ODI did not show a significant difference between two groups, 1 month postoperative VAS of the group I (3.2±0.8) was significantly lower than that of the group II (6.1±0.9) (P<0.05). At the last follow-up, the patients did not report a significant difference in the intensity of back pain (VAS; 3.5±1 in the group I and 4±0.9 in the group II, respectively, P=0.69). In terms of ODI, the scores at 1 month follow- up were 54.9%±9.8% in the group I and 72.8%±6.8% in the group II, which showed a statistical difference (P<0.01). Moreover, these difference persisted until the last follow-ups (ODI; 56.1%±9.5% and 60.2%±5.9% in the group I and II, respectively, P<0.05) (Fig. 3).
Radiomorphological results
Mean Inter- and intra-observer kappas for radiomorphological parameters were 0.59 (SD, 0.07) and 0.55 (SD, 0.08), respectively. Ten patients suffered from subsequent fractures following the surgery or initial diagnosis for spinal pathologic fractures during the follow-up period. Three patients showed subsequent fractures just adjacent to the previously affected segment. However, subsequent fractures occurred at skipped segments in 7 patients. Even though baseline height loss (group I, 38.5%±18.1%; group II, 36%±9.1%) and kyphotic angle (group I, 12.2°±7.7°; group II, 12°±4.9°) of the affected vertebrae did not show significant differences, restoration of the vertebral height and local kyphosis were successfully achieved through augmentation procedures. Moreover, the restoration of height (27.6%±12.1%) and local kyphosis (11.7°±5.5°) in the group I were superior to that (height loss, 40.6%±11.8%; kyphotic angle, 16°±5.5°) of the group II at the last follow-up (Fig. 4). Among the 48 augmented vertebrae, cement leakage was noted in 10 vertebrae (20.8%) on postoperative CT scans. Leakage into the adjacent disc was the most frequent pattern (5 vertebrae). Leakages into the paravertebral (4 vertebrae) and the epidural (1 vertebra) spaces were also noted. In 20 patients (71%) of the group I, radionuclide scans including bone scan and SPECT were done. Fifty eight vertebrae were diagnosed as a pathologic fracture with the evidence of morphological change at plain radiographs and signal change at MRIs. Among 58 vertebrae, 50 vertebrae (86.2%) showed abnormal uptake at the radionuclide images.
Complications related to the surgery
Even though bone cement leakage occurred in 10 out of 49 augmented vertebrae, there was no leakage leading to clinical symptoms or revision surgery. No other complications related to the surgery such as infection, embolism, bleeding or neurologic deficit occurred in any patient.
DISCUSSION
Multiple myeloma, one of hematologic malignancies is known to have high incidence of skeletal related events such as pathologic fracture or spinal cord compression by epidural myeloma (2, 13, 14). As myelomatous cells have a predilection for bone and peculiar characteristics on host bone, osteolytic lesion and subsequent mechanical failure of the involved bone are some of the major clinical manifestations of multiple myeloma (3, 4, 5, 6, 7). Among these SREs, spinal pathologic fractures are the most common problem. Decreased mobility, neurologic complications, kyphotic posture and respiratory compromise are subsequent problems following multiple spinal fractures besides pain due to mechanical failure. Bisphosphonates and radiotherapy have been tried to reduce and treat the clinical manifestations related to SREs in addition to systemic therapy for multiple myeloma (8, 16).
Surgical interventions also have roles in the spinal involvement of multiple myeloma. However, surgical interventions are limited by the general conditions of the patients, osteoporotic conditions of the bone and multiplicity of the lesions. Therefore, open stabilization and/or decompression is reserved and considered only for the patients with neurologic compromises. Minimally invasive internal stabilization of the affected vertebra using the bone cement has many advantages and is known to have supportive evidences for painful osteoporotic spinal fractures or other spinal pathologic fractures (6, 7, 17, 18, 19). However, there are few studies comparing this with other treatment modalities (7). Moreover, as the bone cement augmentation procedures are not free of complications, repeated procedures at the multiple segments are more likely to result in adverse effects such as complications resulting from bone cement leakage or systemic complications.
Therefore, surgical intervention including bone cement augmentation procedures should be considered in the selected patients. For this clinical decision, level of the affected vertebra may be one of important factors to be considered. The thoracolumbar or lumbar spine may need more mechanical support than the thoracic spine. On this background, authors are prone to recommend surgical intervention in this retrospective series. This would be one of limitations of this study and further studies are required to address this hypothesis.
In terms of clinical results assessed using VAS and ODI, these bone cement augmentation procedures presented immediate pain relief (superior VAS at 1 month in the treated group). And these results are similar to those of other studies (18, 20, 21). Moreover, clinical results representing back disability (ODI) at the last follow-up showed significant differences between two treatment groups. Even though most patients experienced an early pain relief after the procedures, the patients suffered from kyphotic postural change and decreased pulmonary capacity at the long-term follow-ups. These clinical manifestations might contribute the differences of VAS and ODI at the last follow-up. Radiological changes including local kyphosis and height loss of the involved vertebra might be also related to these clinical results. However, since whole spine alignment was not evaluated in the present study, further studies on relationship between clinical results and global sagittal spinal alignment are expected to address this issue. In the surgery group, restoration of radiomorphological changes of the affected vertebrae was well maintained during the follow-up. However, as mentioned above, gradual kyphosis of posture, loss of height and decreased pulmonary capacity due to multiple compression fracture are major complaints of the patients at the follow-ups. In general, survival rate of the myeloma patients with pathologic fractures is about 20% lower than that of the patients without pathologic fractures (22). Survival rate in this study did not show a significant difference between two treatment groups. Although this study does not have enough cohort number to evaluate a significant survivorship, considering that main complications leading to death are infections including pneumonia, prevention of kyphosis and preservation of pulmonary capacity would be important for the long-term clinical results. Therefore, further studies are needed to explain that intervention of the fractures involving the thoracic spine could influence the maintenance of pulmonary capacity, and the long-term clinical results.
Basically, a cold spot or negative finding on radionuclide scan such as bone scan and SPECT is known to be related to the behaviors of myelomatous cells which decrease osteoblasts activity and increase osteoclasts activity (23, 24). However, in our series, uptake of the affected vertebrae was noted in 86.2% of the morphologically fractured vertebrae at the initial radionuclide studies. False positive vertebrae were not noted in any patient. The radionuclide studies were initially planned to be helpful for determining the augmented segments. And the findings of these radionuclide studies were considered for selective augmentations for the patients with the myeloma spinal fractures. We could not get firm evidences of clinical efficacies of this clinical pathway with this study. However, on surgical decision for selection of the augmentation lesions, considering the involved levels (such as the thoraco-lumbar or lumbar) and radionuclide studies may be helpful. Further studies including comparative studies could present more reliable evidences.
As the myelomatous cells are known to be highly sensitive to radiotherapy, radiotherapy is preferred modality to manage the clinical manifestations of multiple myeloma. However, the patients who underwent radiotherapy for the spine lesions were excluded in this study. Although several studies have reported the clinical efficacy of radiotherapy for spinal pathologic fractures by myeloma, clinical usefulness of radiotherapy is to treat neurologic problems or prevent the pathologic fractures rather than to treat the pathologic fractures. In addition, the purpose of this study is to investigate the efficiency of treatment for spinal pathologic fractures. Therefore, we excluded the patients who received radiotherapy. However, authors also agree that radiotherapy should be considered for lesions with epidural extensions, and recommend this primarily. Interestingly, subsequent problems such as further collapse or occurrence of epidural myeloma at the initial lesions were not noted in both groups of the study. These clinical courses were quite different from authors' cases of epidural myeloma (25). These findings made the authors hypothesize that clinical courses of the epidural or extra-skeletal myeloma may be quite different from myeloma presenting pathologic fractures without epidural myeloma.
The retrospective design, relative small cohort and short follow-up (16.8 months) are limitations of this study. However, this study presents the clinical efficacy and safety of bone cement augmentation procedures for spinal pathologic fractures of multiple myeloma. Moreover, selective augmentation considering the involved level and findings of radionuclide studies could be useful for surgical decision making. Although these surgical treatments could present immediate pain control and good surgical results, patients have complained of postural changes (kyphosis) and decrease of pulmonary cavity over time. Further prospective study should include these clinical aspects as assessment items.
In conclusion, during the 16.8 months follow-up, bone cement augmentations for spinal pathologic fractures related to multiple myeloma presented efficient short-term pain relief compared to the conservative treatments. Radionuclide studies were useful in detecting pathologic fracture, and provided some information for surgical decisions. Selective bone cement augmentation procedures by considering the involved level and radionuclide studies may provide efficient surgical outcomes and reduce the surgical burdens.




 XML Download
XML Download