

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
An automated liquid culture system is one of the major achievements in tuberculosis (TB) diagnostics. It increases the case yield by 10% over solid media and reduces the diagnostic delay (1, 2). However, liquid media are more prone to bacterial contamination and isolation of nontuberculous mycobacteria (NTM) (3). In addition, some strains grow only on solid media. Therefore, the current international guidelines have recommended the combined use of liquid and solid media on all specimens to maximize sensitivity (4, 5). However, this recommendation was primarily based on studies with respiratory specimens.
Pleural effusion cultures using solid media have been considered minimally helpful for the diagnosis of TB pleurisy in clinical practice because of their low sensitivity and diagnostic delay (6). The yield of effusion culture has increased considerably by implementation of liquid culture methods (7, 8, 9, 10, 11). However, previous studies were too heterogeneous to quantify the impact of liquid media in the diagnosis of HIV-uninfected patients with TB pleurisy.
We conducted a head-to-head comparison of liquid and solid media in effusion culture in order to evaluate how much the diagnostic yield is increased in HIV-uninfected patients by implementation of the liquid culture system, as compared to solid media. This study also aimed to assess whether the combined use of liquid and solid media is necessary to maximize the sensitivity of effusion culture and to determine the predictors of culture-positive effusion.
MATERIALS AND METHODS
Subjects and data collection
We included consecutive patients with TB pleurisy who underwent diagnostic thoracentesis at the Pusan National University Yangsan Hospital, Korea, from January 2011 to December 2013. An automated liquid culture system was introduced in the hospital in August 2010, and was routinely performed in combination with solid media on all specimens from January 2011. If patients could not expectorate sputum spontaneously, sputum induction was performed according to the standardized protocol.
We retrospectively reviewed the patients' medical records for collection of demographic, radiological, and microbiological information. The initial chest radiographs and computed tomography (CT) scans were reviewed by a blinded radiologist. The amount of pleural effusion was graded as small, moderate, or large based on the chest radiographs before thoracentesis (12).
Diagnostic criteria
A definitive diagnosis of TB pleurisy was made if one of the following criteria were met: 1) positive mycobacterial culture in pleural fluid or pleural biopsy tissue samples; 2) granulomatous inflammation in pleural biopsy tissue samples; 3) positive mycobacterial culture of sputum and pleural effusion that was resolved with anti-tuberculous treatment. TB pleurisy was considered probable in patients with lymphocytic exudates from the first or subsequent thoracentesis, high pleural fluid ADA levels (>40 U/l), negative cytological results, and effusions that cleared in response to anti-TB treatment.
Laboratory methods
Pleural fluid was collected into 50 mL sterile polypropylene tubes and transported to the laboratory. Pleural fluid samples were concentrated by centrifugation without decontamination procedures. The pellet was resuspended in 1-2 mL of sterile phosphate buffer (pH 6.8), and both Ziehl-Neelsen- and auramine-stained smear were examined. About 0.5 mL of sediment was cultured using the BACTEC MGIT 960 system (MGIT) (BD Diagnostic Systems, Sparks, MD, USA) according to the manufacturer's instructions, and another 0.5 mL was inoculated onto the Ogawa medium (Korean Institute of Tuberculosis, Seoul, Korea). The Ogawa media were incubated under an atmosphere containing 5% CO2 at 37℃ and were observed on a weekly interval till 8 weeks, whereas the MGIT were processed till 6 weeks.
Statistical analysis
The chi-square test or Fisher's exact test was performed to compare categorical variables, and Student's t-test or Mann-Whitney U-test was used to compare continuous variables. To identify the predictors of positive effusion culture, binary logistic regression analysis with the backward elimination method was performed for variables with P<0.2 in the univariate analysis, and the Hosmer-Lemeshow test was used to test the goodness-of-fit of the models. All analyses were performed using SPSS version 15.0 (SPSS Inc, Chicago, IL, USA), and results with P<0.05 were considered statistically significant.
RESULTS
Diagnosis of tuberculous pleurisy
A total of 104 patients with TB pleurisy were included in this study. The mean age of the patients was 50 (range 16-96) yr, and 59 (56.7%) of them were male. HIV-ELISA tests were performed on 24 patients, and all were sero-negative.
Among the 104 patients, 76 (73.1%) were diagnosed as definite TB pleurisy, while the remaining 28 (26.9%) were probable TB pleurisy. The sensitivity of each method for the diagnosis of TB pleurisy is presented in Table 1. The sensitivity of effusion culture was 41.3%, which was about five times higher than that of TB-PCR (8.4%). The combination of the effusion and sputum cultures contributed to a good diagnostic yield of 66.3% (69/104), while 25 (24.0%) patients were culture positive with regard to the pleural fluid alone. Medical thoracoscopic biopsy was performed on 20 patients, all of whom showed granuloma or were culture positive on pleural tissue samples.
Comparison of culture media in effusion culture
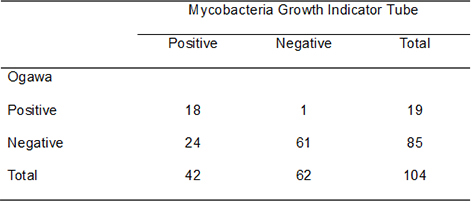
Of the 104 pleural fluid samples, 43 (41.3%) were culture positive on either the MGIT or the Ogawa media. The culture yield of MGIT was higher (40.4%, 42/104) than that of Ogawa media (18.3%, 19/104) (P<0.001) (Table 2). One pleural fluid sample was positive only in the Ogawa medium. The median time to positivity was faster in the MGIT (18 days, range 8-32 days) than in the Ogawa media (37 days, range 20-59 days) (P<0.001). No contamination or growth of NTM was observed on either of the culture media.
Predictors of culture-positive effusion
Patients with culture-positive effusion were younger than those with culture-negative effusion; however, there were no significant differences in other demographic characteristics (Table 3). The number of patients with lung infiltration on chest CT was higher while the number of patients who showed sputum-smear positivity was lower in the effusion culture-positive group than in the effusion culture-negative group. However, these differences were not statistically significant (P=0.171 and P=0.099, respectively). With regard to pleural fluid findings, patients with culture-positive effusion had significantly lower lymphocyte percentage, pH, and glucose level, and higher polymorphonuclear leukocytes (PMNL) percentage and LDH level than patients with culture-negative effusion.
The multivariate logistic regression model identified three independent predictors of the culture-positive effusion, including effusion PMNL percentage (aOR 1.026; 95% CI 1.006-1.046), effusion pH level (aOR 0.06; 95% CI 0.005-0.757), and effusion LDH level (U/l) (aOR 1.002; 95% CI 1.001-1.003) (Table 4).
DISCUSSION
This study aimed to evaluate the impact of the implementation of automated liquid culture systems on the diagnosis of TB pleurisy. The results showed that the use of automated liquid culture systems can provide approximately twice as high yields and fast results in effusion culture in HIV-uninfected patients, as compared to those obtained using solid media. Effusion culture provided a confirmatory diagnosis in about 40% of patients when liquid media alone were used, and in nearly two thirds of the patients when combined with sputum culture. Although effusion culture using solid media has been considered minimally helpful because of its low sensitivity, the role of effusion culture should be reconsidered with the implementation of the automated liquid culture system. Mycobacterial culture remains the gold standard for the detection of and drug susceptibility tests in TB pleurisy. The higher yield obtained using liquid culture media may facilitate early and adequate treatment, consequently improving the outcome of patients with TB pleurisy.
Studies using liquid media reported approximately 40%-60% of sensitivity in effusion culture (7, 8, 9, 10, 11). However, previous studies were too heterogeneous to quantify the impact of liquid media in the diagnosis of HIV-uninfected patients with TB pleurisy. Some of these studies did not directly compare the performance of liquid and solid media (7, 10, 11), included HIV-infected patients who often show higher yields in effusion culture (10, 11), or used bedside inoculation (7, 8, 11). In one study, the BACTEC system provided positive cultures in 24% of HIV-negative patients and 75% of HIV-positive patients (9). Studies using bedside inoculation of pleural fluid showed higher sensitivity of mycobacterial culture than that observed with laboratory inoculation (7, 8, 11). Due to the heterogeneity of these studies, it is still unclear how much the diagnostic yield is increased in effusion culture in an HIV-uninfected patient population with the implementation of the liquid culture system as compared to solid media. The approximately 40% yield of effusion culture was comparable to the values reported in previous studies in consideration of an HIV-uninfected patient population and using the laboratory inoculation in this study.
The major limitations of using liquid culture in respiratory specimens were higher contamination rate and higher isolation of NTM, which often has an ambiguous clinical significance. In addition, some of the strains grew only on the solid media. Due to the above reasons, supplemental solid media have been recommended to maximize culture sensitivity. In this study, no contamination or NTM isolation was observed on solid or liquid media from pleural fluid. Pleural effusion samples are sterile, and therefore, less likely to be contaminated than respiratory samples. In addition, one of the effusion samples grew only on the Ogawa medium. The combined use of liquid and solid media increased the sensitivity only by a further 1% when compared to that observed using the liquid medium alone. Although supplemental solid media showed little effect on maximizing sensitivities in effusion culture in this study, further large-scale studies are required in this regard.
Another interesting finding of this study is the fact that a higher percentage of PMNL is an independent predictor of culture-positive effusion. This finding is consistent with those of previous studies using solid or liquid media (10, 13, 14). It has been suggested that PMNL-rich effusion appears in early phase, when the immune system has not yet developed an effective defense against the bacillus (14, 15). The proportion of PMNL-dominant effusion was reported to be about 10% of TB pleurisy (16), which was related to higher mortality mainly because of delayed diagnosis (13, 17). If TB pleurisy is suspected but unlikely due to a higher percentage of PMNL, the collection of sputum and pleural fluid samples for mycobacterial culture should be encouraged.
This study has inherent limitations because of the small sample size and retrospective study design. Therefore, further studies to validate our findings are warranted. Further, HIV-ELISA tests in this study were only performed on 24 patients. Since Korea is a low-HIV burden country with a reported prevalence below 0.1% (18), the HIV-ELISA test is not a routine test for patients with suspected tuberculosis. None of the patients included in this study were diagnosed with HIV infection during the follow-up period.
In summary, when compared with solid media, an automated liquid culture system could generate approximately twice as high yields and fast results in effusion culture in HIV-uninfected patients. Such diagnostic improvements could facilitate adequate patient treatment, and potentially diminish the morbidity and mortality resulting from TB pleurisy. Supplemental solid media appears to have a limited impact in maximizing sensitivity in effusion culture; however, further studies are warranted.

 XML Download
XML Download