

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The advances in early detection and treatment of cancer have contributed to extend the lives after cancer diagnosis. The five-year survival rate of cancer patients occurring from 2006 to 2010 was 64.1% for the Korean population (1). The National Cancer Data Base and the Surveillance, Epidemiology, and End Results (SEER) and Medicare Database of the USA show that nearly 13.7 million Americans were living with cancer in 2012 and the size of cancer survivors is predicted to increase to nearly 18 million by 2022 (2).
The cancer survivors tend to have greater risks for the secondary cancers (3, 4) and other chronic health problems such as hypertension, diabetes mellitus, and cardiovascular disease (5), in addition to the potential risk of primary cancer recurrence. In addition to the genetic factors and cancer treatment related factors, the behavioral factors such as smoking, alcohol, physical activity, and nutritional factors have been found to contribute to the increasing health risks of the cancer survivors (2, 6, 7, 8).
Among the health behaviors, cigarette smoking is the most important modifiable risk factor for cancer- and non-cancerrelated morbidity and for the mortality of cancer patients (2, 9). The persistent smoking after cancer diagnosis has been known to deteriorate long term outcome, reduce the efficacy of cancer treatment, increase the risk of secondary cancers, and reduce the quality of life for cancer survivors (4, 6, 8, 10, 11, 12). Although smoking cessation has been known to be beneficial to health even after cancer diagnosis (8, 12), many cancer survivors continue to smoke (13, 14, 15, 16).
The previous studies found that the factors associated with persistent smoking after cancer diagnosis were younger age (15, 17, 18), sex (18), lower level of education (15, 19), unmarried status (15, 19), alcohol use (17, 20), type of cancer (15, 17), high nicotine dependency (19, 21), multiple attempts to quit smoking (17), and exposure to second-hand smoking (22). However, most of these studies are limited to the survivors of head and neck cancer or lung cancer in the western population (17, 20, 23) and Asian study was scarcely conducted (14). Up until now, only one study on the Korean patients was conducted in a hospital setting (14), which may lack representativeness.
In this regard, we conducted this study using the nationwide survey data in order to figure out the patterns of smoking behavior and the factors that are associated with persistent smoking of the cancer survivors.
MATERIALS AND METHODS
Study participants
The study participants were Korean men and women over 19 yr of age who participated in the Korean National Health and Nutrition Examination Surveys (KNHANES) from 2007 to 2011. The KNHANES is a cross-sectional nationwide community health survey conducted by the Korea Center for Disease Control, in order to investigate the health and nutritional status of children and adults in Korea. The survey selected representative sample from all ages of Korean population using a stratified, multistage probability sampling design.
Methods of measurement
The KNHANES is composed of three parts: health interview survey, health examination, and nutrition survey. All measurements were conducted by well-trained medical personnel. Health survey and measurements were conducted in specially designed and equipped mobile centers, whereas nutrition survey was conducted by visiting each household selected for the survey. Laboratory tests were conducted using fresh blood drawn after a minimum of 8 hr of fasting. Using structured questionnaire, the following information were collected: information on demographics of the residential area, level of education and income, economic activity, marital status, health history (cancer, cardiovascular disease, diabetes mellitus, and depression), subjective stress, health habits (smoking, alcohol use, and physical activity), and presence of smoker in the household.
Grouping of subjects by parameters
Among 42,347 participants of the KNHANES from 2007 to 2011, 871 people reported to have been diagnosed with cancer. Of the 871 people, 130 people who were smokers at the time of cancer diagnosis were identified for this study using the information about 'lifetime smoking', 'current smoking', 'age at cancer diagnosis', 'age at smoking initiation', and 'duration of smoking (for ex-smokers)' collected for the KNHANES (Fig. 1). Subjects with benign tumor, skin cancer, carcinoma in situ, or unclear or ill-defined (malignant or benign) cancer were not considered as cancer survivors. A smoker was defined as a person who has smoked 100 or more cigarettes throughout the lifetime and continued to smoke until the time at cancer diagnosis. For subjects who were identified as cancer survivor, we further checked for the type of cancer and the age at cancer diagnosis. For those with multiple primary cancers, the first diagnosed cancer was included to the analysis. We categorized the following as smoking related cancers: head and neck, lung, esophagus, stomach, pancreas, cervix, bladder, kidney, other genitourinary organ, and leukemia (24). Cancers at the thyroid, thymus, duodenum, liver, gallbladder, biliary duct, colorectum, breast, uterus, ovary, prostate, osteosarcoma, lymphoma, and multiple myeloma were categorized non-related to smoking. We calculated years lapsed after the diagnosis of cancer using the current age and the age at the first cancer diagnosis.
We categorized cancer survivors who were smoking at the time of cancer diagnosis into two groups according to change in smoking status between the time of cancer diagnosis and the time of the survey: quit-smokers (those who stopped smoking after the time of cancer diagnosis and maintained quit-smoking status until the time of survey) and persistent smokers (those who continued to smoke until the time of survey).
As the survey was conducted cross-sectionally, the data on the change in smoking status was reconstructed using information about age at the time of the survey, age at the time of cancer diagnosis, age at the time of starting smoking, and age at the time of quit-smoking.
We collected data on 'high risk alcohol use', which was defined as consuming seven or more standard drinks for males and five or more standard drinks for females at least once a month. In addition, we checked alcohol dependency using Alcohol Use Disorders Identification Test (AUDIT) (25, 26).
We categorized the level of physical activity into 'active' or 'inactive' on the basis of the intensity and expenditure of time. Walking for more than 30 min at a time over five times a week, moderate activities for more than 30 min at a time over five times a week, or vigorous activities for more than 20 min over three times a week were all considered adequate level of activity. Those completing such amount of exercises were categorized into physically 'active' group. Those who do not meet such criteria were included into 'inactive' group.
Residential area was categorized into two groups: urban areas or rural areas. The urban areas include Seoul, the surrounding metropolitan area in Gyeonggi, and other six major metropolitan cities throughout the country. The rural areas include all of the remaining areas. Level of education achieved was categorized into two groups: ≤9 yr or >9 yr of school. We categorized economic activities into two groups: economically inactive or active. The economically inactive group includes the unemployed, housewives, students, and military. We categorized individual incomes into two groups based on quartiles: the bottom 25% or upper 75%. Marital status was categorized into two groups: married or unmarried. If a person has never married, divorced, separated, or widowed, we categorized him or her into the unmarried group. We categorized subjective stress into two levels based on the response to a question, "Are you under stress?": where the participants choose ratings between the minimal to mild or the moderate to severe.
Well-trained research assistants carried out the measurements of heights and weights while the participants wore light indoor clothing without shoes. Body mass index was calculated as the weight (in kilograms) divided by squared height (in meters). A person with body mass index over 25 kg/m2 was classified obese according to the World Health Organization guidelines for Asian people (27).
Diabetes mellitus was defined as having high fasting serum glucose level (≥7 mM/L), taking glucose lowering agents or insulin, or having previous diagnosis of diabetes mellitus. Fasting serum glucose level was measured from fresh blood drawn after a minimum 8 hr of fasting.
Statistical analysis
For the 130 cancer survivors, who were smoking at the time of cancer diagnosis, we further categorized them into two groups according to their smoking status at the time of KNHANES: quit smoker and persistent smoker. We compared characteristics of the quit smokers and persistent smokers using a chi-square test after the direct age standardization. Then, we evaluated the association of each measured variables with the risk of persistent smoking by estimating odds ratio and 95% confidence intervals with or without adjusting for age and sex.
To evaluate factors that have independent association with persistent smoking, we did multiple logistic regression analysis by putting age, sex, and those variables that were found to have a at least borderline significant (P<0.100) association with persistent smoking in age and sex adjusted analysis as covariates. As six subjects had missing values for any of those selected covariates, 124 subjects were finally included in the multiple logistic regression analysis.
We conducted statistical analyses using PASW statistics 21.0 (SPSS Inc., Chicago, IL, USA) with consideration of sampling weights that were provided by the Korea Centers for Disease Control and Prevention to account for the complex survey design of KNHANES. P value less than 0.05 was considered statistically significant for all analyses.
RESULTS
During the time lapse of 7.52 yr (standard deviation=0.34) after cancer diagnosis, 57 (40.4%) of the smoking cancer survivors stopped smoking after the diagnosis of cancer while 73 (59.6%) have continued to smoke. When we looked at the rate of persistent smoking of survivors by specific sites of cancer, all of the lung cancer survivors stopped smoking. However, substantial proportions of survivors from other cancers have persisted smoking (40.5%-100%) without significant difference among them (data not shown).
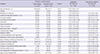
Table 1 shows the associations between the measured variables and the persistent smoking of cancer survivors. Unadjusted analysis showed that low income, high risk alcohol use, physical inactivity, moderate to severe stress, short (<10 yr) time lapse after cancer diagnosis, and presence of smoker in the household were significantly associated with persistent smoking. When age and sex were adjusted, the findings from unadjusted analysis did not materially change for the most variables. However, a positive association between the duration of smoking and persistent smoking became evident with an age and sex adjustment.
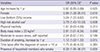
Table 2 shows findings from multiple logistic regression analysis with full adjustment for the covariates. In this analysis, female, low income, high risk alcohol use, high body mass index (≥25 kg/m2), presence of smoker in the household, and longer duration of smoking were positively associated with the increased risk of persistent smoking of cancer survivors. Older age was associated with decreased risk of persistent smoking. Physical inactivity, stress, and time lapse after the diagnosis of cancer were not associated with persistent smoking.
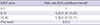
Table 3 shows a relation between AUDIT score and the risk of persistent smoking. We found that high risk alcohol use (AUDIT score≥8) was associated with more than 4 times higher risk of persistent smoking, compared to low to moderate risk alcohol use (AUDIT score<8). Trend test revealed that the higher the AUDIT score the more the cancer survivors continued to smoke (P for trend=0.012).
DISCUSSION
In this study, we evaluated factors associated with persistent smoking of cancer survivors using a survey data of a nationally representative population. A previous study of 142 lung cancer survivors reported that 19% of the survivors who were smoking at the time of cancer diagnosis continue to smoke (23). Other studies found that around 50% of the smokers tended to quit smoking soon after cancer diagnosis, but up to 60% (around 30% of survivor who were smoking at the time of cancer diagnosis) of them restarted smoking later, mostly within 2 months (18, 28, 29). We found that more than 50% of the cancer survivors who were smoking at the time of cancer diagnosis continued to smoke, which is significantly higher compared to the rate of 26.6% of previous Korean studies (14). This unexpectedly high rate of persistent smoking among Korean cancer survivors could be related with the high prevalence of smoking among general Korean population. In addition, relatively low medical attention to smoking cessation for cancer patients in Korea could be a probable reason (30). Another probable reason could be the different distribution of cancer types in this study compared to other studies. The participants in our study survived a wide range of cancer types while the participants of other previous study survived only the smoking related cancers. Finally, differences in the interval between the time of cancer diagnosis and time of survey between the previous study (2.4 yr) and our study (7.4 yr) can be another possible reason.
We found that younger cancer survivors were more likely to smoke persistently than older survivors. This is consistent with the finding that smoking prevalence in general population tends to decrease with increasing age (31). Given that cumulative rate of successful smoking cessation increases over time through the repeated attempt to quit smoking, the older cancer survivors may be more successful to quit smoking. In addition, the older cancer survivors tend to have more chronic diseases than the younger survivors, which could further encourage the older survivors to quit smoking (16).
The associations between sex and smoking behavior after the diagnosis of cancer were controversial in the previous studies (13, 15, 17, 20). However, we found that the females have risk about six times higher, even after adjusting for other health habits and socioeconomic factors. Several reasons can be taken into consideration. We suppose that this finding is attributable in part to the higher proportion of the cervical cancer survivors included in our study. The cervical cancer survivors occupied 8.2% of our study subjects, which is very high compared to the proportion of cervical cancer among the total cancer patients (4.0% in 2012) registered by the Korea Central Cancer Registry (1). The cervical cancer survivors were found to have the highest smoking rate and are less likely to quit smoking (15, 16, 32). Females are less likely to quit smoking among the general population (33) and this tendency is also applied to female cancer survivors.
We found that low income was associated with persistent smoking of Korean cancer survivors, which is consistent with the findings of other studies (28, 34). Time and financial constraints for receiving preventive health services including smoking cessation programs may be the hindrance for the low income population. According to the cross-sectional design of our study, we could not negate the lower willpower of persistent smokers compared to successful quitters, and its strong correlation to the low income.
Previous studies showed that smoking and drinking behaviors were closely related to each other in the cancer survivors (17, 20). Smokers, of general population, with heavy alcohol use tend to have higher nicotine dependency (31), so these were the ones having greater difficulty with smoking cessation among the cancer survivors, which is compatible with the findings for general population (14, 19, 20). This is consistent with our study as well. However, it is still unclear why the smoking and alcohol use are closely associated with each other. As a probable reason, those two were considered to give a psychological benefit to cope with stress. When we examined AUDIT score that is frequently used to identify people with alcohol dependency in our study subjects, we found that the higher the AUDIT score the more the cancer survivors continued to smoke (P for trend=0.012). Given that the combined use of cigarette and alcohol after treatment of cancer has negative synergic effects on the occurrence of a second neoplasm (19), healthcare professionals should provide cancer survivors who smoke persistently with information about the negative health-related outcomes.
In this study, the presence of smokers in the household was associated with 8-times higher risk of persistent smoking. It is remarkable that about 15% of the family members of cancer survivors were smoking, and the proportions of household members' smoking is similar between the cancer survivors and the subjects without cancer. Weaver et al. (28) also found that 24.5% of the family members of lung cancer patients and 19.7% of the family members of colorectal cancer patients were current smokers. Smoking behaviors are found to be affected by intra-familial smoking for the general populations (18). Household members who smoke tends to hinder the lung cancer patients' motivation toward smoking cessation (21, 35). Kashigar et al. (22) reported that smoking behavior of a spouse has important influence on smoking cessation in head and neck cancer patients. These findings suggest that cooperative support by family members of the cancer survivors, such as tailored intra-familial support and smoking restriction at home, is important to lead cancer survivors to quit smoking.
The strength of our study is that study subjects were selected from the representative samples of Korean population for a nationwide community health survey. The crude prevalence of previous cancer diagnosis found in this study (781/42,347 persons) is comparable to the cancer prevalence of among Korean population (2,190 per 100,000 persons in 2011) reported by the Korea National Cancer Information Center (1), which supports the representativeness of our study.
Our study has some limitations. First, the small number of cancer survivors included in the study did not provide enough power for subgroup analysis by sex, age group, or cancer types. However, we could identify factors that have significantly strong association with persistent smoking. Second, we used data collected by self-administered questionnaire. This could have resulted in under-reporting of undesirable behaviors such as smoking or alcohol use, and may have caused underestimation of the risk association. Identifying the cancer survivors by self-report may be less accurate compared to the reviewing of medical record or the health care data. Third, KNHANES is a cross-sectional study, which does not allow prospective observation. We have overcome this problem by reconstructing the time sequencing using related information and could examine longitudinal change in smoking status over 7.52 yr (standard deviation=0.34) after cancer diagnosis. However, even with this effort, we could not clearly identify those who have repeatedly quit and restarted smoking and there could have been some misclassification bias. In addition, some smokers at the time of cancer diagnosis who restarted smoking just prior to cancer diagnosis after a long time of quit-smoking and re-quit smoking before the time of survey participation could have been erroneously classified as quit-smokers at cancer diagnosis and excluded from the present study, because their age at quit-smoking was calculated by adding the duration of smoking to their age at smoking initiation.
Fourthly, the information about stages of cancer, cancer treatment, and recurrence were not available in KNHANES data, and we could not evaluate the effects of these factors on persistent smoking of the cancer survivors. Finally, this study could not provide information about cancer survivors with advanced diseases because the target populations of KNHANES were community residents, and the institutionalized patients were not included in the survey.
In conclusion, this study found that many of the cancer survivors continued to smoke even after the cancer diagnosis. Several factors such as female, low income, high risk alcohol use, obesity, presence of smoker in the households, and longer duration of smoking were associated with the increased risk of persistent smoking in cancer survivors. These findings suggest that more efforts for smoke cessation should be in place for the cancer survivors with increased risk of persistent smoking.

 XML Download
XML Download