

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Sudden unexpected death in epilepsy (SUDEP) is the most common direct epilepsy-related cause of death in patients with epilepsy (1). Although in most patients with epilepsy, seizures are controlled well with medical treatment of conventional and new antiepileptic drugs (AEDs), SUDEP does occur in some patients with epilepsy. The pathophysiologic mechanism of SUDEP may include paroxysmal autonomic dysfunction such as cardiac problems or respiratory distress (2, 3, 4), but there is no clearly established consensus while the physiological mechanism remains unclear. Without established explanations for SUDEP, the analysis of possible risk factors becomes important to predict and reduce the risk of SUDEP. Despite all efforts to identify risk factors from descriptive epidemiologic studies, identifying factors that predict SUDEP is still challenging.
Many previous studies have reported that early onset, male gender, duration of epilepsy, polytherapy, nocturnal seizures, and generalized tonic clonic seizures (GTCS) are among the significant risk factors for SUDEP (5, 6, 7, 8, 9, 10, 11, 12); however, these studies were performed in western populations and there are few data if Asian patients with epilepsy have the same risk factors for SUDEP as western patients with epilepsy. The purpose of this study was to explore the association between patient characteristics and SUDEP in patients with epilepsy in Korea, focusing mainly on risk factors that have been identified by previous investigators.
MATERIALS AND METHODS
Subjects and study design
The subjects in this study were patients who were registered and treated for epilepsy at Asan Medical Center, University of Ulsan College of Medicine, Korea, the tertiary hospital in Korea, between 1993 and 2011. A total of 35,638 patients with epilepsy were enrolled. Epilepsy was defined as a history of two or more unprovoked seizures or a single seizure with evidence of epileptiform activity recorded by electroencephalogram or structural lesions documented by brain imaging. Medical records of patients were reviewed in detail and information on the cause of death was collected from the National Statistics Office database, which is matched to the hospital records using the unique national identification number of each patient.
Inclusion criteria
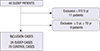
Cases were individuals who had died, had a diagnosis of epilepsy registered on the death certificate and were treated for epilepsy at our center in the study period, and met the criteria for SUDEP. SUDEP was defined according to Leestma et al. (13) using the following criteria: 1) Patient has the disease of epilepsy, 2) unexpected death occurred while the patient was in a reasonable state of health, 3) death was sudden, 4) death occurred during normal activities and benign circumstances, 5) there was no evidence of an obvious medical cause of death, and 6) death did not occur as a result of direct insult of status epilepticus or seizure. SUDEP is typically classified as definite if an autopsy has been performed and probable if no autopsy has been performed (14). In Asian countries such as Korea, cultural customs and habits mean that is not common to perform an autopsy, so all SUDEP patients in the present study were classed as probable SUDEP. To ensure that we only included cases with identifiable clinical course over a long period, we excluded cases that were followed for less than 5 yr. We also excluded cases aged <5 yr or >70 yr, because unexpected death in these age groups may have many differential causes (Fig. 1). All included subjects were receiving AED stationary at least more than 1 yr. Forty-six patients met the SUDEP criteria and were considered for inclusion in the study.
Eleven were excluded due to short duration of follow up (<5 yr) and a further nine were excluded due to age (Fig. 1). Finally, 26 SUDEP patients were included as cases in this study. Control subjects were living epilepsy patients matched for age, sex, and initial date of enrollment at our medical center. Three control participants were included for each case. For all subjects, demographic and clinical characteristics were extracted from the medical records, including age, age at seizure onset, disease duration, sex, family history of epilepsy, the presence or absence of psychiatric problems (depression or anxiety), seizure frequency during the recent 1 yr (≤1 per month, >1 per month), the classification of epilepsy (generalized idiopathic, symptomatic partial, cryptogenic partial, undetermined). And further information were collected including the presence or absence of aura, the presence or absence of seizure associated lesions on MR images (focal cortical dysplasia, epilepsy associated tumor, polymicrogyria, medial temporal sclerosis), the number of AEDs, and the type of AEDs used.
Statistical analysis
Demographic and clinical characteristics were compared between cases and controls using an independent t-test for continuous variables and a chi-square test for categorical variables. Univariate logistic regression analysis was used to identify demographic and clinical characteristics associated with SUDEP. Characteristics that were significant in the univariate analysis were entered into a multivariate regression analysis to identify those that were independently associated with SUDEP. All statistical analyses were performed using SPSS (version 21.0; SPSS Inc., Chicago, IL, USA), with statistical significance defined as an alpha level <0.05. Data are reported as mean±standard deviation or No. (%).
RESULTS
Subject characteristics
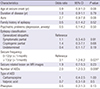
Twenty-six SUDEP cases and 78 controls were included in the study. General characteristics of the cases and controls are shown in Table 1. The age of SUDEP cases and controls was 41.5±11.3 yr and 41.2±11.4 yr, respectively. The age at seizure onset was 19.6±15 yr and 22.7±13 yr, respectively, and disease duration was 22.7±11.5 yr and 22.3±8.7 yr, respectively. Male gender was more predominant (65%) and familial history of epilepsy was about 5 percent in both groups. Psychiatric problems like depression or anxiety were evaluated because of worse effects on quality of life (QOL) (15) and occupied 5% in both groups. These characteristics were similar in the two groups.
Seizure frequency was <1 per month in 11 of the 26 SUDEP cases (42.3%) and >1 per month in 15 of the 26 SUDEP cases (57.7%). Seizure frequency was <1 per month in 53 of the 78 controls (65.4%) and >1 per month in 25 of the 78 controls (34.6%). This was statistically different between two groups (P=0.035). The number of AEDs used was also more in SUDEP cases compared with controls (2.0±1.1 vs. 1.4±0.7, P=0.02).
Epilepsy was classified as idiopathic generalized epilepsy in 5 of the 26 SUDEP cases (19.2%), symptomatic partial epilepsy in 11 of the 26 SUDEP cases (42.3%), cryptogenic partial epilepsy in 5 of the 26 SUDEP cases (19.2%) and undetermined in 5 of the 26 SUDEP cases (19.2%). Epilepsy was classified as idiopathic generalized epilepsy in 12 of the 78 controls (15.4%), symptomatic partial epilepsy in 26 of the 78 controls (33.3%), cryptogenic partial epilepsy in 10 of the 78 controls (12.8%), and undetermined in 30 of the 78 controls (38.5%). Epilepsy classification was not significantly different between two groups.
Seizure-related lesions were observed in 10 of the 23 SUDEP cases with magnetic resonance images (50%) and 33 of the 75 controls with magnetic resonance images (42.3%). The proportion of patients with seizure-related lesions was similar in the two groups.
Risk factors for SUDEP
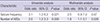
The univariate analysis using conditional logistic regression showed that seizure frequency (odds ratio: 3.1; P=0.021) and number of AEDs (odds ratio: 2.0; P=0.009)were significantly associated with SUDEP (Table 2). Only the number of AEDs remained significant in multivariate analysis (odds ratio: 1.83; P=0.026; Table 3). No individual AED was significantly associated with SUDEP (Table 2).
DISCUSSION
The main findings of the present study were that epilepsy patients who died from SUDEP had a significantly higher frequency of seizures and used significantly more AEDs than living epilepsy patients, suggesting that seizures were more severe in epilepsy patients who died from SUDEP. Consistent with previous studies, a higher seizure frequency and polytherapy were significantly associated with SUDEP in univariate analysis, and only polytherapy remained associated with SUDEP in multivariate analysis (11, 16, 17). Although higher number of AEDs were the variable most strongly associated with SUDEP in this study, it is controversial whether polytherapy should be avoided to reduce risk of SUDEP, because the association is not necessarily causal, but results and polytherapy may simply be a marker of severe epilepsy (14). Our findings suggest that disease severity, as represented by uncontrolled seizures and polytherapy, may be an important risk factor for SUDEP.
The number of AEDs used ranged from one to four and many patients were treated with valproic acid, carbamazepine or phenytoin. Although the mechanism and pathophysiology of SUDEP is not clearly understood, unstable cardiac function has been postulated as a cause (5, 18). Several studies have proposed that AEDs harm cardiac function by arrhythmia or QT prolongation, which may then cause SUDEP (19, 20, 21). We found no association between the type of AED used (carbamazepine, valproic acid, phenytoin) and SUDEP, which supports previous studies and suggests that individual drugs were not likely to cause SUDEP (21, 22).
There are controversies as to whether or not epilepsy classification is associated with SUDEP (10, 11, 13, 17). In the present study, we did not find any association between epilepsy type and SUDEP. This may be partially due to the relatively high proportion of patients with undetermined epilepsy in the present study and other supportive data such as brain magnetic resonance images and electroencephalogram that were normal.
Seizure frequency is a well-known risk factor for SUDEP, but recent studies reported that seizure frequency of GTCS is much more important than for patients with any other type of seizure (1, 8). However in our study, because many of the included patients lived alone and could not remember or describe the semiology, it was difficult to discriminate whether the type of seizures was GTCS or not in all included patients.
This study has several limitations. First, it was retrospective and may involve selection bias. In several patients it was not possible to determine the type of epilepsy, and data on the presence of nocturnal seizures and the time of SUDEP were not available due to the paucity of medical records or the unknown history. Second, we included patient with epilepsy who were followed up for at least 5 yr because of stable clinical condition and compliance of medication. However, by including more patients with confirmed diagnosis of epilepsy may gain stronger power. Third, we studied patients who were treated at the Asan Medical Center as early as1993, and many patients were treated with conventional AEDs such as valproate, carbamazepine and phenytoin. Small numbers of patients were treated with new AEDs such as lamotrigine, topiramate, oxcarbamazepine and levetiracetam, and our data therefore provide limited information on the association between new AEDs and SUDEP. Additional cohort studies of patients treated with new AEDs are necessary to evaluate the relation between new AEDs and SUDEP. Finally as seizure frequency and number of AED may have high interaction, careful interpretation is needed in our result.
In conclusion, we found that a higher frequency of seizures and the number of AEDs were associated with SUDEP, which may suggest that the severity of epilepsy is associated with SUDEP, regardless the type of AED used.

 XML Download
XML Download