

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Neurological complications of human immunodeficiency virus (HIV) infection are common, even in the era of effective antiretroviral treatment (ART) (1). Seizures and epilepsy are important neurological complications. HIV infection carries a higher risk of seizures due to the risk of opportunistic infections of the central nervous system (CNS) (2). In addition, HIV has direct, harmful effects on the CNS (2), and primary CNS infection itself appears to be the cause of some seizures (3). Moreover, in addition to direct neurological complications due to HIV or other infections, medications used for HIV therapy (3, 4, 5) and metabolic abnormalities (2, 6) may predispose HIV patients to seizures.
Studies of seizures and HIV infection have been performed retrospectively (2, 7, 8, 9, 10), prospectively (11, 13) or in a large cohort (1). The prevalence of seizures is estimated to be between 1% and 11% in adult patients with HIV infection (1, 2, 7, 9, 12). However, most studies have investigated white, black or Indian patients, and few studies have examined clinical features of seizures among HIV-infected patients in Korea (13).
We retrospectively investigated the prevalence, etiology and clinical aspects of seizures in adult Korean patients with HIV infection.
MATERIALS AND METHODS
Study population and variables
We retrospectively reviewed the records of consecutive HIV-infected patients older than 18 yr of age at a single infectious disease clinic at the National Medical Center in Seoul, Korea, between January 2008 and December 2013. We included patients who had experienced at least one seizure after becoming infected with HIV and patients who had developed epilepsy before becoming infected with HIV. The diagnosis of seizures or epilepsy was verified, and patients with inconclusive histories or incomplete medical records that prevented a diagnosis of seizures or epilepsy from being verified were excluded.
The clinical data recorded for each patient included the age at the time of the first seizure, sex, latency between the diagnosis of HIV infection and the first seizure, immunological status (most recent CD4 counts) at the time of the first seizure and HIV treatments being administered at the time of the first seizure. We determined the probable etiologies of seizures based on the presence of CNS diseases, laboratory abnormalities or other provocative factors (e.g., drugs). In addition, we categorized individual etiologies according to the revised ILAE (International League Against Epilepsy) classification (14, 15). Clinical details on the seizures (the frequency and classification of the seizures), EEG data, brain imaging (CT or MRI) data, and the response to antiepileptic drugs were also recorded for each patient. We identified patients with a history of status epilepticus (SE), which is defined as at least 5 min of continuous seizure activity or two or more seizures with an incomplete recovery of consciousness in between (16).
After becoming infected with HIV, the patients with new-onset seizures were divided into two groups according to seizure frequency and severity: patients who had previously had a single seizure and patients who had previously had multiple (≥2) seizures or a history of SE. We regarded patients as having had 'a single seizure' when there was a history of single-episode seizure before the end of the study. We investigated the clinical differences between the two groups for the following dichotomous variables: 1) the most recent CD4 counts (above 200 cells/mL vs. below 200 cells/mL); 2) the presence or absence of epileptiform discharges on EEG; 3) the presence or absence of CNS disease; 4) the presence or absence of cerebral lesions on brain imaging; and 5) the outcome (mortality) during the follow-up period. Not all patients underwent thorough evaluations, and there are discrepancies in the available data for each variable.
Statistical analysis
Comparisons were made between the group of patients who had experienced a single seizure and the group of patients who had experienced multiple seizures or one or more episodes of SE using univariate analysis for each dichotomous variable. We identified the risk factors associated with seizure recurrence or severity using chi-squared tests (with 2×2 cross tabulation).
RESULTS
Patients and seizure etiologies
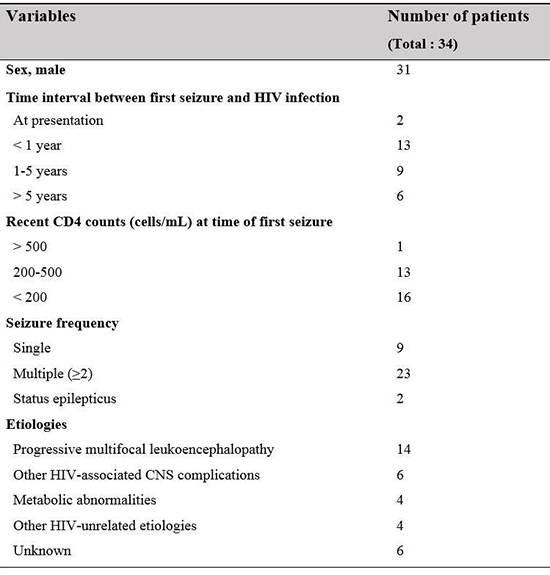
A total of 1,141 HIV-infected patients were reviewed in this study. Of them, 34 (3%) had a history of seizures or epilepsy. A total of 4 of the 34 patients had epilepsy before HIV infection, whereas 30 experienced new-onset seizures. Among the 34 patients, 31 were men, and 3 were women. All patients except one were Korean; the remaining patient was a black person from Cameroon. For the patients with new-onset seizures, the mean age at the time of the first seizure was 46.9 (25-77) yr. The mean latency between HIV diagnosis and the first seizure was approximately 3 yr for the patients with new-onset seizures, and 2 patients had experienced seizures as a presenting manifestation of HIV infection. Most patients had moderate (200-500 cells/mL, n=13) or low (<200 cells/mL, n=16) CD4 cell counts; the mean CD4 cell count was 208.7 cells/mL (range, 6-500 cells/mL). However, the majority of the patients (28 of 30) were being treated with combination antiretroviral therapy (cART) at the time of the first seizure. The demographics and clinical characteristics of the patients are shown in Table 1. The etiologies are listed in Table 2. Acute symptomatic seizures occurred in 6 patients, and remote symptomatic seizures occurred in 22 patients. The most frequent etiology was progressive multifocal leukoencephalopathy (PML, 14 patients), followed by other CNS infections (6 patients) and metabolic abnormalities (4 patients).
In patients with CNS etiologies related to HIV, 8 had experienced early seizures (occurring within 4 weeks of CNS disease onset), and 11 had experienced late seizures. Among the 14 patients with PML, 9 had experienced late-onset seizures. No reason for the seizures was identified in 6 patients, other than HIV infection (unknown etiology). In the 4 patients with a history of seizures prior to HIV infection, the etiologies were cerebral hemorrhage (2 patients), hippocampal sclerosis and cortical dysplasia.
Characteristics of seizures
Among the 34 patients with a history of seizures or epilepsy, 9 (26%) had experienced only a single seizure until the end of study, 23 had experienced two or more seizures, and 2 had experienced status epilepticus. In the 9 cases of a single seizure, the etiologies of 3 cases were remote symptomatic etiologies (2 were PML, 1 was Tb meningoencephalitis), 2 cases involved acute symptomatic etiologies (metabolic abnormalities: septic shock and hepatic encephalopathy), and 4 cases were attributed to an unknown etiology. With the exception of 1 patient, the mean follow-up period after a seizure episode was approximately 23.9 months for patients with a single seizure. The remaining patient died several days after the seizure occurred. One patient had experienced only simple partial seizures, whereas 10 patients had experienced only complex partial seizures. Partial seizures with secondary generalization were observed in 11 patients. A total of 12 patients had experienced only generalized seizures without historical evidence of ever having experienced partial seizures. Electroencephalography (EEG) data were available for 28 patients, and brain-imaging data were available for 32 patients. A total of 10 patients had epileptiform discharges evident on the EEG, and 8 exhibited slow activity without epileptiform discharge. A total of 12 patients had focal or diffuse lesions on brain CT or MRI, and 10 failed to present a lesion (Table 3).
Treatment
Among the patients with new-onset seizures after HIV infection (n=30), 12 (40%) were not treated with anticonvulsants because they had experienced only a single seizure without remote CNS disease or only a single, acute symptomatic seizure (e.g., due to metabolic insults). In contrast, most of the patients with CNS disease or who had experienced multiple, unprovoked seizures were received anticonvulsants. Most seizures responded to one (14 patients) or 2 antiepileptic drugs (8 patients). All patients with epilepsy before HIV infection (n=4) were on anticonvulsant therapy. Levetiracetam was given to 17 patients and was the most frequently prescribed anticonvulsant, followed by valproic acid, which was given to 7 patients.
Most patients had favorable outcomes for the seizures and did not experience any significant additional illness resulting from the seizures. However, two patients with SE died from complications related to their treatment for SE. One patient died of sepsis secondary to a drug-induced coma, and another patient died of a cardiac arrhythmia and hypotension during an infusion of fosphenytoin. The etiologies of SE were CMV (cytomegalovirus) encephalitis and PML. Both of these patients had low CD4 cell counts (70 and 174 cells/mL). During the follow-up period, seven patients died of infections related to immune deficiency and unrelated to their seizures.
Frequency of seizures
Patients who had experienced multiple seizures or SE more commonly had brain-related seizures or epilepsy etiologies than did those who had experienced only one seizure (P=0.019). In addition, epileptiform discharges on EEG were more frequently present in patients who had experienced multiple seizures or SE (P=0.032). There was a trend toward the presence of cerebral lesions on brain imaging in patients with a history of multiple seizures or SE (15 of 21) compared to those who had experienced only one seizure (3 of 7), but this difference was not significant (P=0.172). No relationship was found between seizure frequency and CD4 count (P=1.000) or between seizure frequency and mortality (P=0.794) (Table 4).
DISCUSSION
To the best of our knowledge, this is the first report of the relationship between seizures and HIV infection in the Korean population. We found that the prevalence of seizures and epilepsy was higher in the HIV population than in the general population. A recent study of the general Korean population reported that the prevalence of epilepsy was 2.41/1,000 persons (17). In this study, the prevalence of seizures in HIV-seropositive patients was approximately 3% (34/1,141). Only 4 of 1,141 patients had epilepsy before HIV infection; this prevalence is similar to that found in a general population study. Two earlier studies reported a significantly higher prevalence of seizures, at 11% (7) and 17% (18), but a more recent study, conducted after the introduction of ART, reported a lower prevalence of approximately 1% (1).
Prior to their first seizure, 16 (53%) of the 30 patients with new-onset seizures had CD4 counts below 200 cells/mL and were considered to have AIDS. The CD4 count is a risk factor for most CNS infections associated with HIV typically when it is below 200 cells/mL. Seizures in HIV-positive patients occur mainly during the late stages of infection, when intracranial pathology is more commonly found (25). However, compared with previous studies in which the percentage of patients with AIDS has ranged from 54.5% to 84% (2, 7, 11, 12, 19), our study sample exhibited a relatively low incidence of AIDS. In addition, prior to the start of seizures, the majority of patients had already been receiving cART and had a median duration of HIV infection of 3 yr. Thus, in our series, a considerable number of patients were not in an advanced stage of immune suppression. The majority of seizures were associated with remote symptomatic etiologies caused by underlying brain lesions rather than acute symptomatic etiologies (acute CNS insults, which may be acute structural, metabolic, toxic, infectious, or due to inflammation); the latter may be more commonly attributed to systemic illness or impaired immunological status (15).
Two patients had seizures as a first clinical symptom of HIV infection. Seizures have previously been reported as a presenting manifestation of HIV infection (3, 10, 20).
We were able to identify the cause of seizures in 28 of 34 (82%) patients. The seizures in these patients had brain etiologies (with the exception of 4 patients who had metabolic abnormalities), and the leading cause of seizures was PML (14 patients). A total of 6 patients had other opportunistic infections. These results differ from previous findings that CNS toxoplasmosis and HIV-associated encephalopathy were the most common causes of HIV-related seizures (2, 3, 7, 10, 12). The reason for this discrepancy may be that toxoplasmosis is a very rare complication of HIV in Korea (21, 22).
Although PML is considered to be restricted to the white matter, seizures in patients with PML and HIV have frequently been reported (23, 24). The pathogenic mechanisms underlying seizures in PML are unclear. The lesions immediately adjacent to the cortex can act directly as excitatory foci and are associated with the occurrence of seizures (24). Moreover, neurons whose axons have been damaged may become hyperexcitable, potentially initiating the development of seizures (24).
No definitive etiology other than HIV infection itself was found in 6 patients. This result is consistent with those of previous studies. New-onset seizures in HIV without a discernible etiology is considered a nonspecific manifestation of HIV encephalopathy (2, 3, 7, 25, 26). Postmortem examinations of the brain have demonstrated the presence of microglial nodules and multinucleated giant cells, both of which are features of HIV encephalopathy (7). Thus, direct HIV infection of the brain is considered to be responsible for seizures in these individuals (3).
Most patients with multiple seizures or remote CNS disease received anticonvulsants. In our study, levetiracetam was the most commonly prescribed anticonvulsant because it has a broad spectrum of activity, and its metabolism does not involve the enzymes of the cytochrome P450 system (28). Recent guidelines have stated that it is important to avoid enzyme-inducing anticonvulsants in people on antiretroviral regimens, as pharmacological interactions may cause virological failure (28).
Most seizures were not intractable and did not cause severe medical complications. These findings are consistent with more recently published reports (2, 8). However, 2 patients with SE had fatal complications associated with the treatments that they received for seizures. Previous studies have found higher mortality (29%) and morbidity (36%) for SE in the HIV population (26). SE often occurs in patients with advanced HIV disease, and patients who died had lower CD4 counts than did those who survived (26). Our study also found that both patients with SE had more advanced HIV disease.
Epileptiform discharges on EEG and the presence of brain disease were significant risk factors for recurrent seizures. These risk factors for recurrent seizures are also observed in the general population (29, 30). Early identification of the risk factors for seizure recurrence is important because recurrent seizures and status epilepticus are associated with significant morbidity and mortality.
The limitations of our study include incomplete neurological evaluations and insufficient analysis of the seizure characteristics, which occurred because this was a retrospective study with most patients being examined in an infectious disease clinic. Because this study was a single-center study, the distribution of HIV-related diseases may differ from the distribution of HIV-related diseases within a larger population.
In summary, seizures are more frequent in patients with HIV infection than in the general population. PML was the most common seizure etiology in the patients investigated in our study, and most of the seizures, with the exception of SE, had favorable outcomes. Seizure recurrence and the development of epilepsy are associated with the presence of brain disease and EEG abnormalities.


 XML Download
XML Download